
Abstract
Objective
To evaluate modified anterior abdominal wall cervicopexy (AWC) as a less invasive (via 3-cm minilaparotomy) and more augmented (via securing posterior vaginal wall to uterosacral ligaments) technique.
Methods
Case series of 30 women with Stages III and IV apical uterine prolapse assessed by the pelvic organ prolapse quantification system.
Results
The modified AWC procedure was performed successfully for 17 cases with Stage III uterovaginal prolapse and 13 cases with Stage IV uterovaginal prolapse. The procedure was conducted safely with no operative or postoperative complications, apart from two cases with postoperative urinary retention. Operative time ranged from 45 to 70 min. Follow-up was available for 1–3 years. Overall, 27 cases were satisfied with the procedure, and three cases developed recurrence after caesarean section due to cutting the supporting sutures
May 2017 · Volume 6 · Issue 5 Page 1777
International Journal of Reproduction, Contraception, Obstetrics and Gynecology
Rameshkumar R et al. Int J Reprod Contracept Obstet Gynecol. 2017 May;6(5):1777-1781
www.ijrcog.org pISSN 2320-1770 | eISSN 2320-1789
Original Research Article
Modified purandare’s cervicopexy-a conservative surgery for genital prolapse: a retrospective study
Rameshkumar R., Leena Kamat*, Spoorthi Tungal, Suma Moni
INTRODUCTION
Nulliparous prolapse is reported to account for 1.5% to 2% of all cases of genital prolapse in Indian population.1 The incidence rises to 5%-8% for young women who have delivered one or two children, making it the highest in the world. The high prevalence of this condition in India can be attributed to malnutrition, poor socioeconomic status and deliveries conducted by untrained dais at home. As this type of prolapse occurs at a younger age, the surgical technique should not only reduce the prolapse but also retain the reproductive function. Various conservative surgeries have been described in the past, each having their own merits and de-merits.
Purandare described a technique for the surgical treatment of genital prolapse in young women in 1965.2
Department of Obstetrics and Gynecology, SDM College of Medical Sciences and Hospital, Manjushree Nagar, Sattur, Dharwad, India
Received: 11 March 2017
Revised: 15 March 2017
Accepted: 30 March 2017
*Correspondence:
Dr. Leena Kamat,
E-mail: kamatleena082@mail.com
Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT Background: Purandare described a technique for the surgical treatment of genital prolapse in young women in 1965. This technique of cervicopexy is easy to perform and provides dynamic support to the uterus. The objective of study is to evaluate the role of modified Purandare’s cervicopexy in the treatment of genital prolapse in reproductive age group and to study the pregnancy outcome and fertility in patients who have undergone modified Purandare’s sling surgery. Methods: Between January 2007 and December 2015, 20 women in the reproductive age (mean age 30.5 years, range 24 to 37 years) underwent modified Purandare’s cervicopexy at Shree Dharmasthala Manjunatheshwara (SDM) College of Medical Sciences, Dharwad, India. Of these, 2 (10%) patients were nulligravida, 7 (35%) were primipara and 11 (55%) were multigravida. Four (20%) women had associated infertility. Additional surgeries like tubectomy were performed in 4 (20%) women, tubal patency test in 3 (15%), ovarian drilling in 2 (10%) and myomectomy in 2 (22.2%) women, and cystocele repair was done in 4 women (20%). Results: All 20 patients were analysed for intraoperative and postoperative complications. All were followed up for mean duration of 12 months. There were no reported intra or post-operative complications. Out of 4 infertile women, 2 conceived spontaneously 6 months after the surgery. Of these, one delivered successfully at term by lower segment caesarean section and other by normal vaginal delivery. One woman conceived 8 months after the surgery spontaneously, antenatally followed for 3 months and then later was lost to follow-up. There was no recurrence of prolapse. Conclusions: Nulliparous prolapse can be treated by various surgical procedures, each having their own merits and de-merits. Our modification of Purandare’s cervicopexy is simple, effective and is less technically demanding.
Keywords: Cervicopexy, Infertility, Nulliparous prolapse
DOI: http://dx.doi.org/10.18203/2320-1770.ijrcog20171529
Rameshkumar R et al. Int J Reprod Contracept Obstet Gynecol. 2017 May;6(5):1777-1781
International Journal of Reproduction, Contraception, Obstetrics and Gynecology Volume 6 · Issue 5 Page 1778
This technique of cervicopexy is easy to perform and provides dynamic support to the uterus. In this study, we present the operative results of 20 cases of genital prolapse in young women, treated by modified Purandare’s cervicopexy technique. METHODS The objectives of present study are to evaluate the role of modified Purandare’s cervicopexy in the treatment of genital prolapse in reproductive age group and to study the pregnancy outcome and fertility in patients who have undergone modified Purandare’s sling surgery. Between January 2007 and December 2015, 20 patients with nulliparous prolapse underwent modified Purandare’s cervicopexy at Shri Dharmasthala Manjunatheshwara College of Medical Sciences and Hospital, Dharwad. Prior to surgery all patients underwent clinical examination and Shaw’s classification for staging of the prolapse. Only women with 2nd and 3rd stage genital prolapse were operated. In women with infertility, all other causes for same were ruled out. All women were operated in the post-menstrual phase. Written and informed consent was taken in all patients. Approval from institute’s ethical committee was taken. RESULTS
The average age at the time of operation ranged from 24 to 37 years (mean age-30.5 years) (Table 1). All 20 patients underwent Modified Purandare’s cervicopexy. Out of 20 women, 2 (10%) were nulligravida, 7 (35%) were primiparas and 11 (55%) were multigravida (Table 2).
Table 1: Age distribution of the patients. Age (years) Number Percent < 20 0 0
21-30
11
55 31-40 9 45
> 40
0
0
Table 2: Parity of the patients. Parity Number Percent Nulligravida 2 10
One
7
35 Two 6 30
Three
4
20 Four and above 1 05
85% of women had come with symptom of mass per vagina. Of the others, 2 patients (10%) had discharge per vagina, 2 patients (10%) had backache, 3 patients (15%) had pain abdomen and 4 patients (20%) had infertility (Table 3).
Table 3: Presenting complaints. Complaints Number Percent Mass per vaginum 17 85
Discharge per vagina
2
10 Backache 2 10
Pain abdomen
3
15 Infertility 4 20 Mean duration of occurrence of prolapse after delivery was 4 years. 15 % of the prolapse occurred within one year of child birth, 65% occurred within 3 years of child birth (Table 4).
Table 4: Distribution of patients according to duration between delivery and prolapse. Duration between delivery and prolapse (year) Number Percent <1 1 5
1
2
10 2 4 20
3
4
20 4 or more 7 35 Women with second and third degree of prolapse were operated. 60% had third degree prolapse (Table 5). 35% patients had concomitant cystocele, 15% patients had enterocele and 25% had concomitant rectocele (Table 6).
Table 5: Distribution according to degree of genital prolapse. Degree of prolapse Number Percent Second degree 8 40
Third degree
12
60
Table 6: Concomitant organ prolapse. Number Percent Cystocele 7 35
Enterocele
3
15 Rectocele 5 25
Average duration of the surgery was 1 hour 30 minutes to 2 hours (mean 1 hour and 50 minutes). Additional surgeries like tubectomy was performed in 4 (20%), tubal patency test in 3 (15%), ovarian drilling in 2 (10%), and myomectomy in 2 (10%), cystocele repair in 4 (20%) patients (Table 7).
Table 7: Additional surgeries performed. Additional surgery performed Number Percent Tubectomy 4 20
Tubal test
3
15 Ovarian drilling 2 10
Myomectomy
2
10 Cystocele repair 4 20
Rameshkumar R et al. Int J Reprod Contracept Obstet Gynecol. 2017 May;6(5):1777-1781
International Journal of Reproduction, Contraception, Obstetrics and Gynecology Volume 6 · Issue 5 Page 1779
Operative procedure
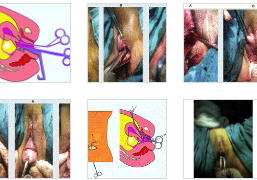
All patients were operated in the post menstrual phase of the cycle, after taking detailed written informed consent. The modified Purandare’s cervicopexy was performed under spinal anaesthesia in low lithotomy position (Figure 1).
Figure 1: Pre-operative picture with prolapse.
Pfannenstiel incision was utilised and the abdomen was opened in layers. Wide exposure of the rectus abdominis muscle was done, maintaining perfect haemostasis (Figure 2).
Figure 2: Wide exposure of rectus muscle.
Uterus was delivered through the incision and held with Shirodkar’s uterus holding forceps. The bladder was dissected inferiorly (Figure 3).
A 25-30 cm long strip of polypropylene mesh was prepared by soaking it in 200 ml normal saline containing amikacin. The mesh was fixed anteriorly at the level of isthmus (Figure 4) by No.1 polypropylene and polyglactin 910 sutures.
Figure 3: Dissection of bladder.
Figure 4: Attaching the mesh to the isthmus.
The ends of the mesh were brought lateral to rectus muscle retroperitoneally on both sides (Figure 5) taking care not to injure the inferior epigastric vessels.
Figure 5: Bringing the mesh lateral to the rectus muscle bilaterally.
Rameshkumar R et al. Int J Reprod Contracept Obstet Gynecol. 2017 May;6(5):1777-1781
International Journal of Reproduction, Contraception, Obstetrics and Gynecology Volume 6 · Issue 5 Page 1780
After confirming the correct fixation and haemostasis the uterovesical fold of peritoneum was approximated. The ends of the mesh were fixed to the rectus muscle by criss crossing (Figure 6) using No 1 polyglactin 910 sutures.
Figure 6. Fixing the mesh to the rectus muscle by criss crossing.
After confirming the haemostasis, the abdomen was closed in layers. Per speculum examination was done to note the reduction of prolapse (Figure 7). Additional procedures like posterior colpoperineorrhaphy, if needed, were performed later.
Figure 7: Postoperative picture.
Patients were monitored for immediate complications like haemorrhage, bladder injury, bowel injury, febrile morbidity and surgical site infection. 19 patients were available for follow up till 24 months after surgery. 1 patient was lost for follow up after 1 year. At each follow up, the patients were assessed for recurrence of mass per vagina, pregnancy and pregnancy outcome.
There were no intraoperative or immediate post-operative complications. All patients recovered postoperatively without any complications (Table 8).
Table 8: Complications. Number Percent Pain 0 0
Discharge per vagina
0
0 Recurrence of prolapse 0 0
All 20 patients were treated successfully without any symptom of recurrent prolapse on follow up. Of the 4 women with infertility, 2 conceived spontaneously 6 months after the surgery. They had uneventful antenatal period and successfully delivered, one by lower segment caesarean section and the other one vaginally. There was no prolapse even after vaginal delivery. One woman conceived 8 months after the surgery spontaneously, antenatally followed for 3 months and then later lost to follow-up. All women were satisfied with the surgical result.
DISCUSSION
The occurrence of genital prolapse in a younger woman can be a cause of infertility and significant morbidity. Various conservative surgeries have been described in the past, each having their own merits and de-merits.3 The Manchester operation, described by Donald and Fothergill, was the first surgery described for nulliparous prolapse.4 Shirodkar VN later modified this by describing uterosacral advancement and preservation of the cervix.5
Next in the evolution of conservative surgery for prolapse many sling surgeries were described which soon became popular because of their simplicity and effectiveness. Initially native fascia like fascia lata and rectus sheath were used which later got replaced by synthetic slings that produce minimal tissue reaction and remain unabsorbed giving lifelong support.1
Failure of conservative surgeries like traditional Fothergill’s or sling surgeries was because of use of native fascia for repair, the same endopelvic fascia that has caused prolapse. The use of synthetic materials like merselene tape and mesh in modern sling surgeries has decreased the failure rates and gives lifelong support.
Purandare’s cervicopexy was first described by Purandare BN.2 He used rectus sheath strips as sling material. It was later modified by Purandare VN and Pravin Mhatre they used Mersilene tape and attached the tape to the isthmus posteriorly instead of anteriorly. Purandare’s cervicopexy is technically easy to perform and provides dynamic support to the uterus.
Modified Purandare’s cervicopexy was performed in 20 patients; all were in reproductive age group. Our modification of Purandare’s cervicopexy has many advantages compared to the original operation which can favourably affect the outcome. First is the use of non-absorbable mesh for anchoring, second is criss crossing of mesh on rectus muscle which provides a space for low
Rameshkumar R et al. Int J Reprod Contracept Obstet Gynecol. 2017 May;6(5):1777-1781
International Journal of Reproduction, Contraception, Obstetrics and Gynecology Volume 6 · Issue 5 Page 1781
transverse incision for caesarean section without compromising the mesh anchoring and retaining the support.
Compared to other sling surgeries like Shirodkar’s or Khanna’s operation, this surgery provides dynamic support, is technically easy to perform and complications like Periosteitis, ureteric and sigmoid injuries are avoided.
Modified Purandare’s cervicopexy improves fertility, doesn’t interfere with vaginal birth and if caesarean delivery is required doesn’t damage the mesh thus reducing the recurrence of prolapse.
With the use of synthetic mesh in Modified Purandare’s Cervicopexy, possibility of infection should be anticipated and steps to prevent this like strict asepsis, soaking mesh in antibiotic solution and prophylactic antibiotics should be adopted.
Anterior wall cervicopexy is more anatomically and physiologically appropriate than other sling surgeries, as suspension of the uterus to the rectus sheath keeps the uterus and vaginal axis in anterior position, which mimics the natural vaginal alignment attained by the contraction of the puborectalis muscle. This also supports the bladder neck and gives protection against iatrogenic stress incontinence.6
In the original Purandare’s surgery the fascial strips created from rectus sheath were used, which were fixed to the anterior surface of the uterus.7 As there were higher failure rates with the use of native tissue synthetic materials were designed.8 In our study we have used polypropylene tape. Polypropylene mesh is flexible; it is inert and ideal for supporting the prolapsed viscera
The original Purandare’s anterior wall cervicopexy has comparable outcome of up to 90% when compared to technically difficult procedures like sacrospinous hysteropexy and sacral hysteropexy. However, our modification of Purandare’s cervicopexy is simpler, less technically demanding and has favourable outcome on long term follow-up, with less no recurrence rates.
In the original Purandare’s surgery, the mersilene tape was fixed to anterior abdominal wall laterally at the site of incision. This would sometimes lead to unintended iatrogenic cutting of the supporting sutures while performing caesarean sections.9 We have modified this by criss-crossing of mesh on rectus muscle, which provides a space for low transverse incision for caesarean section without compromising the mesh anchoring and retaining the support.
Modified Purandare’s cervicopexy is technically a simple surgical procedure for treatment of uterine prolapse in young women who wish to retain their reproductive function. This operation can be performed with less intraoperative complications, good postoperative recovery and less recurrence. CONCLUSION
Many procedures exist for treatment of nulliparous prolapse each with variable complications, technical difficulties, effectiveness and costs. Our modification of Purandare’s cervicopexy is simple, effective and has less technical demands.
Funding: No funding sources
Conflict of interest: None declared
Ethical approval: The study was approved by the Institutional Ethics Committee REFERENCES 1. Virkud A. Conservative Operations in Genital Prolapse. J Obstet Gynaecol India. 2016;66(3):144-8. 2. Purandare VN. New surgical technique for surgical correction of genital prolapse in young women. J Obstet Gynaecol India. 1965:53-62. 3. Dietz V, Schraffordt Koops SE, van der Vaart CH. Vaginal surgery for uterine descent; which options do we have? A review of the literature. Int Urogynecol J Pelvic Floor Dysfunct. 2009;20(3):349-56. 4. Fothergill WE. Anterior colporrhaphy and its combination with amputation of the cervix as a Single Operation. BJOG. 1915;27:146-7. 5. Dastur B, Gurubaxani G, Palnitkar SS. Shirodkar sling operation in the treatment of genital prolapse. BJOG. 1967;74:125-8. 6. Salem HT, Tawfik RM, El Saman AM, Nasr A. Anterior abdominal wall cervicopexy for treatment of stage III and stage IV uterine prolapse. Int J Gynaecol Obstet. 2010;110(2):130-2. 7. Purandare VN, Patel K, Aryan R. Operative treatment of genital prolapse in young women. J Obstet Gynaecol India. 1966;16:53. 8. Banu LF. Synthetic sling for genital prolapse in young women. Int J Gynaecol Obstet. 1997;57(1):57-64. 9. Elsaman AM, Hosam TS, Amin M, Fetih AN, Othman EER, Zahran KM. Modified cervicopexy: a novel, less- invasive technique for Stages III and IV uterine prolapse. Eur J Obstet Gynecol Reprod Biol. 2014;183:159-63.
Cite this article as: Rameshkumar R, Kamat L, Tungal S, Moni S. Modified purandare’s cervicopexy-a conservative surgery for genital prolapse: a retrospective study. Int J Reprod Contracept Obstet Gynecol 2017;6:1777-81..
Conclusions
The modified AWC procedure is less invasive, simple and effective for Stages III and IV uterine prolapse.