| Introduction |
- Epidemiology
- incidence
- third most common non-vertebral fracture pattern seen in the elderly (>65 years old)
- demographics
- 2:1 female to male ratio
- increasing age associated with more complex fracture types
- Pathophysiology
- mechanism
- low-energy falls
- elderly with osteoporotic bone
- high-energy trauma
- young individuals
- concomitant soft tissue and neurovascular injuries
- pathoanatomy
- pectoralis major displaces shaft anteriorly and medially
- supraspinatus, infraspinatus, and teres minor externally rotate greater tuberosity
- subscapularis interally rotates articular segment or lesser tuberosity
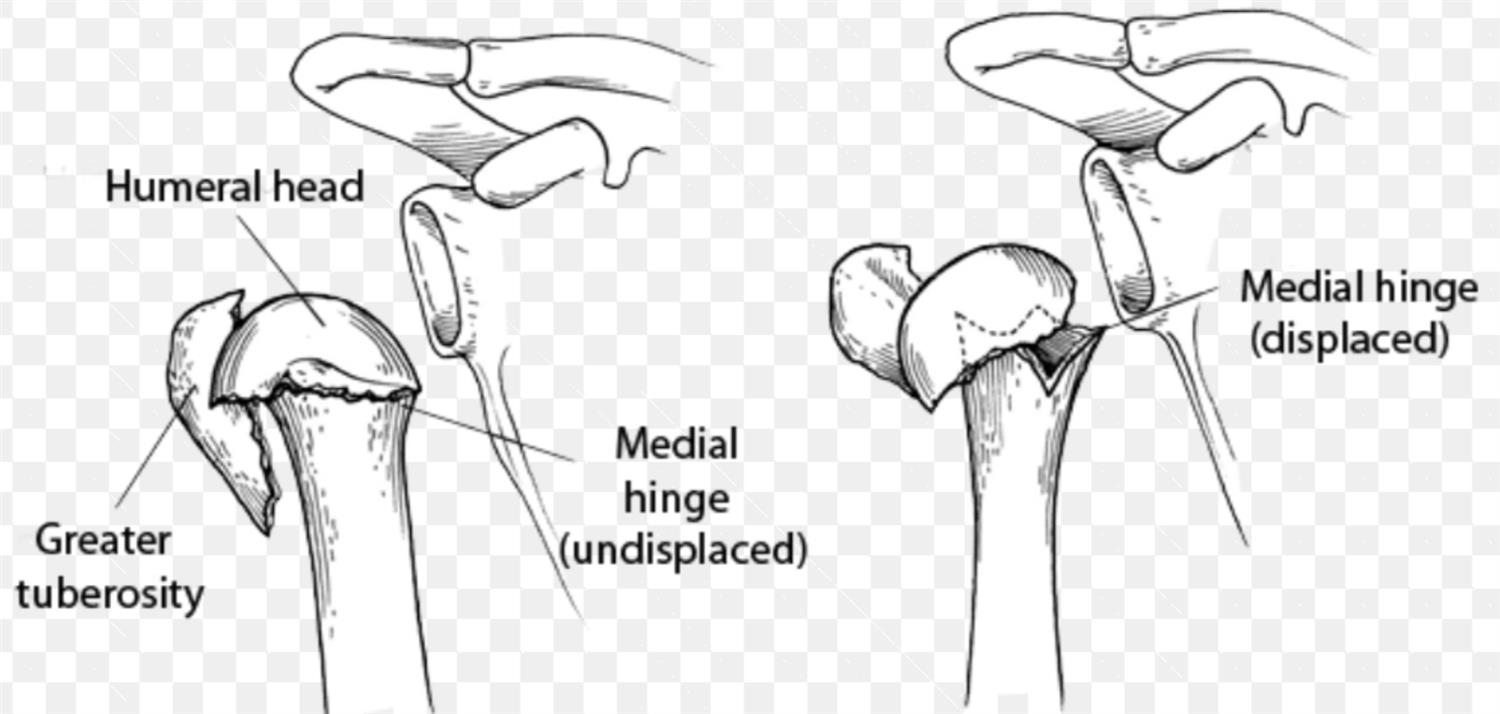
- vascularity of articular segment is more likely to be preserved if ≥ 8mm of calcar is attached to articular segment
 
- 3 most accurate predictors of humeral head ischemia are
- <8 mm of calcar length attached to articular segment
- disrupted medial hinge
- basic fracture pattern
- predictors of humeral head ischemia do not necessarily predict subsequent avascular necrosis
- Associated conditions
- nerve injury
- axillary nerve injury most common
- arterial injury
- uncommon (incidence 5-6%), higher likelihood in older patients
- most often occur at level of surgical neck or with subcoracoid dislocation of the head
|
| Anatomy |
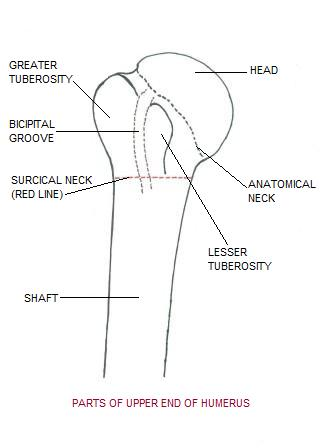
- Osteology
- anatomic neck

- represents the old epiphyseal plate
- surgical neck
- represents the weakened area below head
- more often involved in fractures than anatomic neck
- average neck-shaft angle is 135 degrees
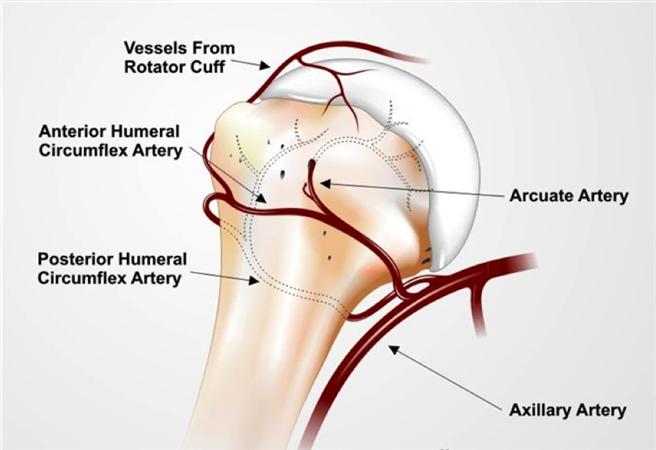
- Vascular anatomy
- anterior humeral circumflex artery

- large number of anastamoses with other vessels in the proximal humerus
- branches
- anterolateral ascending branch
- is a branch of the anterior humeral circumflex artery
- arcuate artery
- is the terminal branch and main supply to greater tuberosity
- posterior humeral circumflex artery
- recent studies suggest it is the main blood supply to humeral head
|
| Classification |
- AO/OTA
- organizes fractures into 3 main groups and additional subgroups based on
- fracture location
- status of the surgical neck
- presence/absence of dislocation
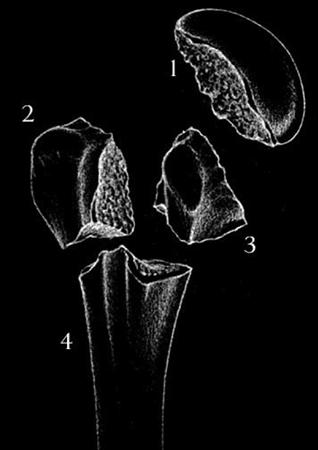
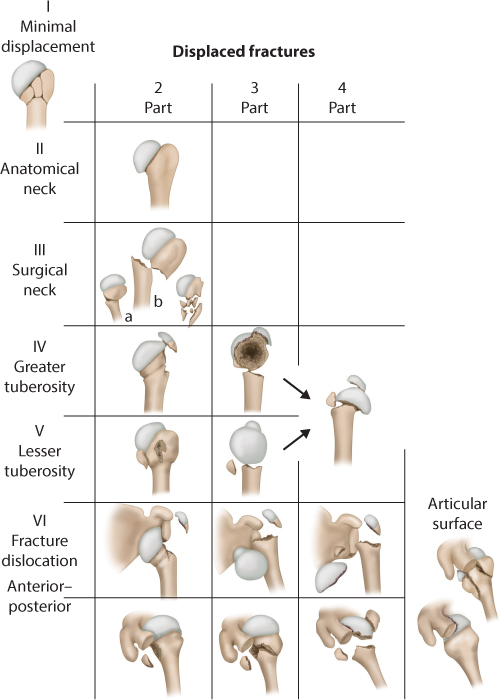
- Neer classification
- based on anatomic relationship of 4 segments
- greater tuberosity
- lesser tuberosity
- articular surface
- shaft
- considered a separate part if
- displacement of > 1 cm
- 45° angulation
|
| Neer Classification |
| |
Minimally
Displaced |
Two Part |
Three Part |
Four Part |
Articular Segment |
| Anatomical Neck |
|
|
|
|
|
| Surgical Neck |
|
|
|
|
|
| Greater Tuberosity |
|
|
|
|
|
| Lesser Tuberosity |
|
|
|
|
|
| Fracture-Dislocation |
|
|
|
|
|
| Head Split |
|
|
|
|
|
|
| Evaluation |
- Symptoms
- pain and swelling
- decreased motion
- Physical exam
- inspection
- extensive ecchymosis of chest, arm, and forearm
- neurovascular exam
- axillary nerve injury most common
- determine function of deltoid muscle (axillary n.)
- arterial injury may be masked by extensive collateral circulation preserving distal pulses
- examine for concomitant chest wall injuries
|
| Imaging |
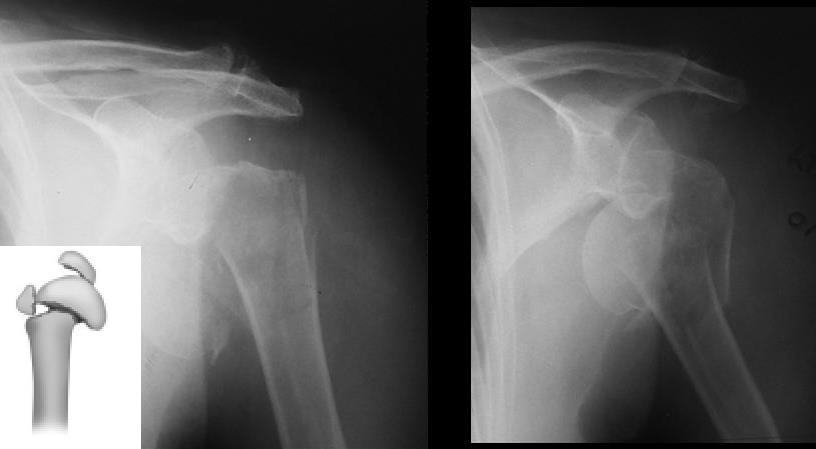
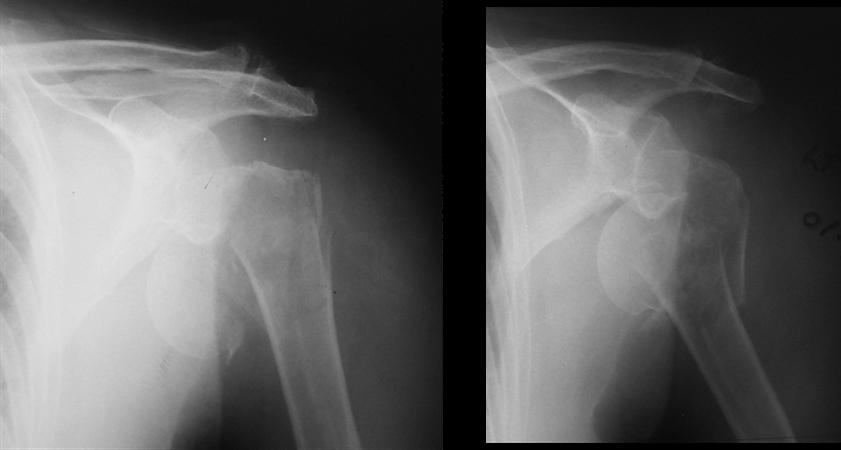
- Radiographs
- recommended views
- complete trauma series
- true AP (Grashey)
- scapular Y
- axillary
- additional views
- apical oblique
- Velpeau
- West Point axillary
- findings
- combined cortical thickness (medial + lateral thickness >4 mm)
- studies suggest correlation with increased lateral plate pullout strength
- pseudosubluxation (inferior humeral head subluxation) caused by blood in the capsule and muscular atony
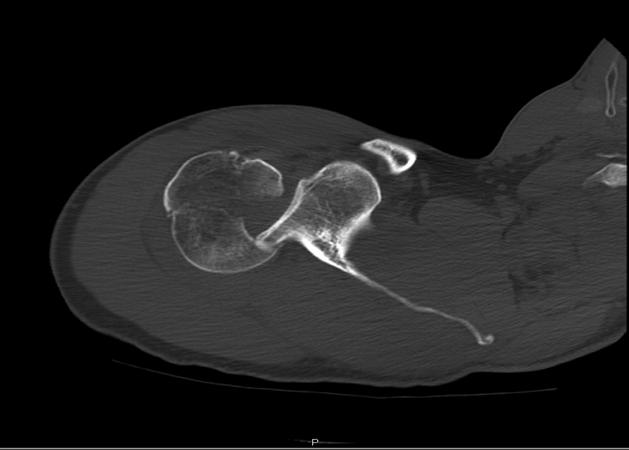
- CT scan
- indications
- preoperative planning
- humeral head or greater tuberosity position uncertain
- intra-articular comminution
- MRI
- indications
- rarely indicated
- useful to identify associated rotator cuff injury
|
| Treatment |
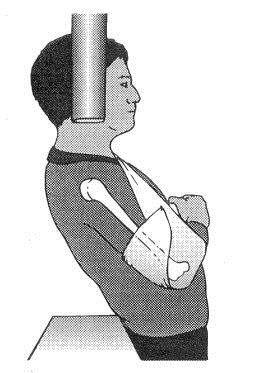
- Nonoperative
- sling immobilization followed by progressive rehab
- indications
- most proximal humerus fractures can be treated nonoperatively including
- minimally displaced surgical and anatomic neck fractures
- greater tuberosity fracture displaced < 5mm
- fractures in patients who are not surgical candidates
- additional variables to consider
- age
- fracture type
- fracture displacement
- bone quality
- dominance
- general medical condition
- concurrent injuries
- technique
- start early range of motion within 14 days
- Operative
- CRPP (closed reduction percutaneous pinning)
- indications
- 2-part surgical neck fractures
- 3-part and valgus-impacted 4-part fractures in patients with good bone quality, minimal metaphyseal comminution, and intact medial calcar
- outcomes
- considerably higher complication rate compared to ORIF, HA, and RSA
- ORIF
- indications
- greater tuberosity displaced > 5mm
- 2-,3-, and 4-part fractures in younger patients
- head-splitting fractures in younger patients
- outcomes
- complication rate higher compared with ORIF
- medial support necessary for fractures with posteromedial comminution
- calcar screw placement critical to decrease varus collapse of head
- intramedullary nailing
- indications
- surgical neck fractures or 3-part greater tuberosity fractures in
- combined proximal humerus and humeral shaft fractures
- outcomes
- biomechanically inferior with torsional stress compared to plates
- favorable rates of fracture healing and ROM compared to ORIF
- arthroplasty
- indications
- hemiarthroplasty
- controversial when considering hemiarthroplasty versus RSA
- younger patients (40-65) with complex fractures or head-splitting components likely to have complications with ORIF
- recommended use of convertible stems to permit easier conversion to RSA if necessary in future
- reverse total shoulder
- low-demand elderly individuals with non-reconstructible tuberosities and poor bone stock
- low-demand patients with fracture dislocation
- outcomes
- improved results if
- accurate tuberosity reduction
- restoration of humeral height and version
- poor results with
- tuberosity nonunion or malunion
- retroversion of humeral component > 40°
|
| Treatment by Fracture Type |
| |
|
Two-Part Fracture
|
|
Surgical Neck
|
• Most common fx pattern
• Deforming forces:
1) pectoralis pulls shaft anterior and medial 2) head and attached tuberosities stay neutral
|
Nonoperative
• Closed reduction often possible
• Sling
Operative
• indications controversial
• technique
- CRPP
- Plate fixation
- IM device
|
|
Greater tuberosity
|
• Often missed
• Deforming forces: GT pulled superior and posterior by SS, IS, and TM
• Can only accept minimal displacement (<5mm) or else it will block ER and ABD
|
Nonoperative
• indicated for GT displaced < 5 mm
Operative
• indicated for GT displacement > 5 mm
- isolated screw fixation only in young with good bone stock
- nonabsorbable suture technique for osteoporotic bone (avoid hardware due to impingement)
- tension band wiring
|
|
Lesser tuberosity
|
• Assume posterior dislocation until proven otherwise
|
Nonoperative
• Minimally or non-displaced
Operative
• ORIF if large fragment
• excision with RCR if small
|
| Anatomic neck |
• Rare |
Nonoperative
• Minimally or non-displaced
Operative
• ORIF in young
• ORIF v. hemiarthroplasty v. reverse total shoulder arthroplasty in elderly
|
|
Three-Part Fracture
|
Surgical neck and GT

|
• Subscap will internally rotate articular segment
• Often associated with longitudinal RCT
|
Nonoperative if:
• Minimally displaced (GT<5 mm; articular segment <1 cm and <45 degrees)
• Poor surgical candidate
Operative:
• Young patient
- percutaneous pinning (good results, protect axillary nerve)
- IM fixation (violates cuff)
- locking plate (poor results with high rate of AVN, impingement, infection, and malunion)
• Elderly patient
- hemiarthroplasty with RCR or tuberosity repair vs. reverse total shoulder arthroplasty
|
| Surgical neck and LT |
• Unopposed pull of posterior cuff musculature leads articular surface to point anterior
• Often associated with longitudinal RCT
|
•Trend towards nonoperative management given high complications with ORIF
• Young patient
- percutaneous pinning (good results, protect axillary nerve)
- IM fixation (violates cuff)
- locking plate (poor results with high rate of AVN, impingement, infection, and malunion)
• Elderly patient
- hemiarthroplasty with RCR or tuberosity repair vs. reverse total shoulder arthroplasty
|
|
Four-Part Fracture
|
Valgus impactedfracture
|
• Radiographically will see alignment between medial shaft and head segments
|
• Low rate of AVN if posteromedial component intact thus preserving intraosseous blood supply
• Surgical technique
1. raise articular surface and fill defects
2. repair tuberosities
|
| 4-part with head-splitting fracture |
• Characterized by high risk of AVN (21-75%)
• Deforming forces:
1) shaft pulled medially by pectoralis
|
• Young patient
- ORIF vs. hemiarthroplasty (hemiarthroplasty favored for nonreconstructible articular surface, severe head split, extruded anatomic neck fracture)
• Elderly patient
- hemiarthroplasty v. reverse total shoulder arthroplasty
|
|
| |
| Techniques |
- CRPP (closed reduction percutaneous pinning)
- approach
- technique
- use threaded pins but do not cross cartilage
- externally rotate shoulder during pin placement
- engage cortex 2 cm inferior to inferior border of humeral head
- complications
- with lateral pins
- risk of injury to axillary nerve
- with anterior pins
- risk of injury to biceps tendon, musculocutaneous n., cephalic vein
- possible pin migration
- ORIF
- approach
- anterior (deltopectoral)

- lateral (deltoid-splitting)
- increased risk of axillary nerve injury
- technique
- heavy nonabsorbable sutures
- (figure-of-8 technique) should be used for isolated greater tuberosity fx reduction and fixation (avoid hardware due to impingement)
- isolated screw
- may be used for greater tuberosity fx reduction and fixation in young patients with good bone stock
- locking plate
- screw cut-out (up to 14%) is the most common complication following fixation of 3- and 4- part proximal humeral fractures and fractures treated with locking plates
- more elastic than blade plate making it a better option in osteoporotic bone
- place plate lateral to the bicipital groove and pectoralis major tendon to avoid injury to the ascending branch of anterior humeral circumflex artery
- placement of an inferomedial calcar screw(s) can prevent post-operative varus collapse, especially in osteoporotic bone
- Intramedullary nailing
- approach
- superior deltoid-splitting approach
- technique
- lock nail with trauma or pathologic fractures
- complications
- rod migration in older patients with osteoporotic bone is a concern
- shoulder pain from violating rotator cuff
- nerve injury with interlocking screw placement
- Hemiarthroplasty
- approach
- anterior (deltopectoral)
- technique for fractures
- cerclage wire or suture passed through hole in prosthesis and tuberosities improves fracture stability
- place greater tuberosity 10 mm below articular surface of humeral head (HTD = head to tuberosity distance)
- impairment in ER kinematics and 8-fold increase in torque with nonanatomic placement of tuberosities
- height of the prosthesis best determined off the superior edge of the pectoralis major tendon (5.6 cm between top of humeral head and superior edge of tendon)
- post-operative passive external rotation places the most stress on the lesser tuberosity fragment
- Reverse shoulder arthroplasty
- approach
- technique for fractures
- ensure adequate glenoid bone stock
- ensure functioning deltoid muscle
- repair of tuberosities recommended despite ability of RSA design to compensate for non-functioning tubersosities/rotator cuff
|
| Rehabilitation |
- Important part of management
- Best results with guided protocols (3-phase programs)
- early passive ROM
- active ROM and progressive resistance
- advanced stretching and strengthening program
- Prolonged immobilization leads to stiffness
|
| Complications |
- Screw cut-out
- most common complication after locked plating fixation (up to 14%)
- Avascular necrosis
- risk factors
- risk factors for humeral head ischemia are not the same for developing subsequent avascular necrosis
- better tolerated than in lower extremity
- no relationship to type of fixation (plate or cerclage wires)
- Nerve injury
- axillary nerve injury most common (up to 58% with studies using EMG)
- increased risk with lateral (deltoid-splitting) approach
- axillary nerve is usually found ~7cm distal to the tip of the acromion
- suprascapular nerve (up to 48%)
- Malunion
- usually varus apex-anterior or malunion of GT
- results inferior if converting from varus malunited fracture to TSA
- Nonunion
- usually with surgical neck and tuberosity fx
- treatment of chronic nonunion/malunion in the elderly should include arthroplasty
- lesser tuberosity nonunion leads to weakness with lift-off testing
- greater tuberosity nonunion leads to lack of active shoulder elevation
- greatest risk factors for non-union are age and smoking
- Rotator cuff injuries and dysfunction
- Missed posterior dislocation (especially in cases with lesser tuberosity fractures)
- Adhesive capsulitis
- Posttraumatic arthritis
- Infection
|