| Introduction |
- Overview
- supracondylar fractures are one of the most common traumatic fractures see in children and most commonly occur in children 5-7 years of age from a fall on an outstretched hand
- treatment is usually closed reduction and percutanous pinning (CRPP), with the urgency depending on whether the hand remains perfused or not.
- Epidemiology
- incidence
- extension type most common (95-98%)
- flexion type less common (<5%)
- demographics
- occur most commonly in children aged 5-7years
- M = F
- Pathophysiology
- mechanism of injury
- fall on outstretched extremity
- Associated injuries
- neuropraxia
- anterior interosseous nerve (AIN) neurapraxia (branch of median n.)
- the most common nerve palsy seen with supracondylar humerus fractures
 
- radial nerve palsy
- second most common neurapraxia (close second)
- ulnar nerve palsy
- seen with flexion-type injury patterns

- nearly all cases of neurapraxia following supracondylar humerus fractures resolve spontaneously
- further diagnostic studies are not indicated in the acute setting
- vascular compromise (5-17%)
- rich collateral circulation can maintain circulation despite vascular injury
- ipsilateral distal radius fractures
|
| Anatomy |
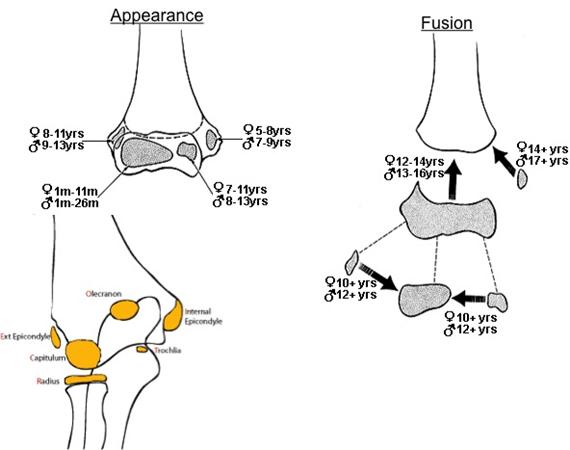
- Ossification centers of elbow
- age of ossification/appearance and age of fusion are two independent events that must be differentiated

- e.g., internal (medial epicondyle) apophysis
- ossifies/appears at age 6 years (table below)
- fuses at age ~ 17 years (is the last to fuse)
|
|
Ossification center
|
Years at ossification (appear on xray) (1)
|
Years at fusion (appear on xray) (1) |
| Capitellum |
1
|
12 |
| Radial Head |
4
|
15 |
| Medial epicondyle |
6
|
17 |
| Trochlea |
8
|
12 |
| Olecranon |
10
|
15 |
| Lateral epicondyle |
12
|
12 |
| (1) +/- one year, varies between boys and girl |
|
| |
| Classification |
| |
|
|
| |
| Presentation |
- Symptoms
- pain
- refusal to move the elbow
- Physical exam
- inspection
- gross deformity
- swelling
- ecchymosis in antecubital fossa
- motion
- limited active elbow motion
- neuro exam
- neurovascular exam must be done before any reduction maneuver to be certain nerve or vascular injury is not iatrogenic (stuck in fracture site)
- Evaluate for
- AIN neurapraxia

- unable to flex the interphalangeal joint of the thumb and the distal interphalangeal joint of the index finger (can't make A-OK sign)
- median nerve injury
- loss of sensation over volar index finger
- radial nerve neurapraxia
- inability to extend wrist, MCP joints, thumb IP joint
- PIP and DIP can still be extended via intrinsic function (ulnar n.)
- vascular exam
- assess pulse
- present or absent by palpation
- present or absent by biphasic doppler pulse
- assess vascular perfusion
- well perfused
- poorly perfused
- cold
- pale
- arterial capillary refill > 2 seconds
|
| Imaging |
- Radiographs
- recommended views
- AP and lateral x-ray of the elbow (really of the distal humerus)
- findings
- posterior fat pad sign

- lucency on a lateral view along the posterior distal humerus and olecranon fossa is highly suggestive of occult fracture around the elbow
- measurement
- displacement of the anterior humeral line
- anterior humeral line should intersect the middle third of the capitellum in children > 5 years old, and touches the capitellum in children in children <5.
- capitellum moves posteriorly to this reference line in extension type fractures and anteriorly in flexion type fractures
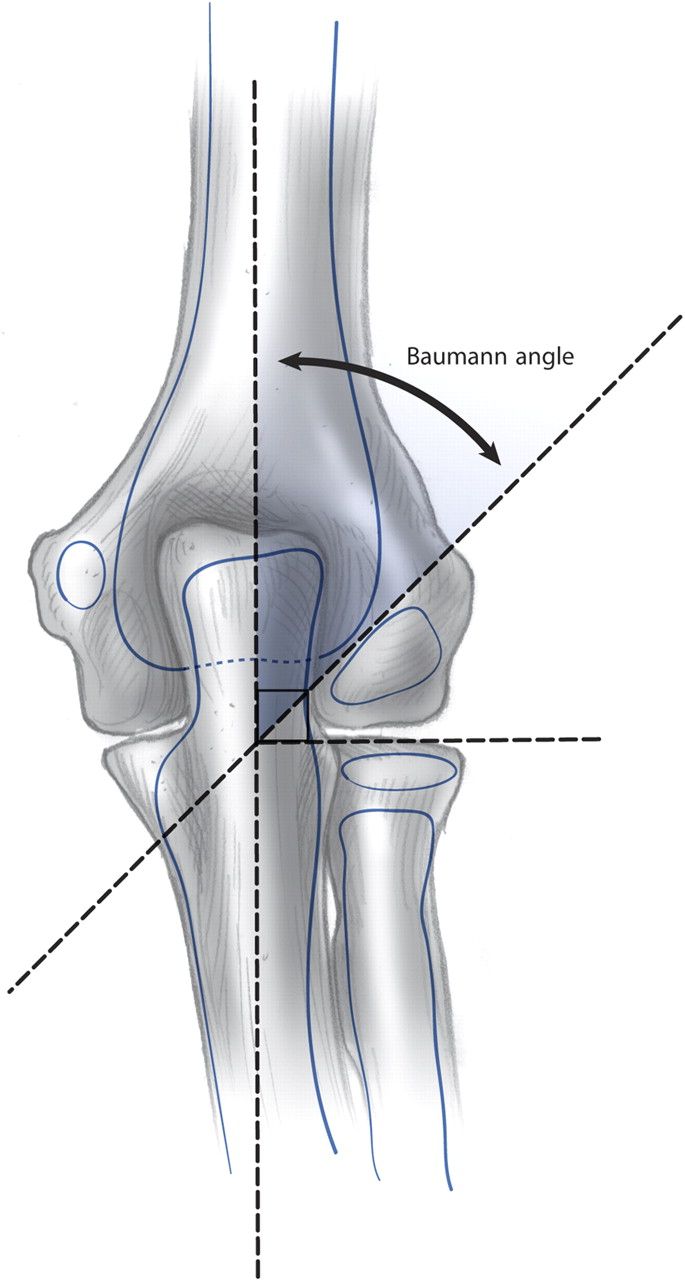
- alteration of Baumann angle
- Baumann's angle is created by drawing a line parallel to the longitudinal axis of the humeral shaft and a line along the lateral condylar physis as viewed on the AP image
- normal is 70-75°, but best judge is a comparison of the contralateral side
- deviation of >5-10° indicates coronal plane deformity and should not be accepted
- Angiography
- is typically not indicated
|
| Treatment |
- Nonoperative
- long arm casting with less than 90° of elbow flexion
- indications
- warm perfused hand without neuro deficits and
- Type I (non-displaced) fractures
- Type II fractures that meet the following criteria
- anterior humeral line intersects the capitellum
- minimal swelling present
- no medial comminution
- technique
- typically used for 3 weeks
- repeat radiographs at 1 week to assess for interval displacement
- immediate bedside closed reduction
- indications
- technique
- gentle traction and elbow flexion to 20-40 degrees
- this often restores perfusion
- if perfusion not restored
- take to OR for CRPP in an urgent or emergent manner (see below)
- if perfusion is restored
- take to OR in an urgent manner
- Operative
- closed reduction and percutanous pinning (CRPP)
- indications
- fracture pattern
- type II and III supracondylar fractures
- flexion type
- medial column collapse
- time to CRPP dictated by neurovascular status
- non-urgent (can wait overnight)
- indications
- warm perfused hand without neuro deficits
- some argue can treat an isolated AIN injury in non-urgent fashion
- technique
- splint in 30-40° elbow flexion, admit overnight for observation and elevation for elective surgery
- urgent (same day - do not wait overnight)
- indications
- pulseless, well-perfused hand
- sensory nerve deficits
- excessive swelling
- "brachialis sign"
- ecchymosis, dimpling/puckering antecubital fossa, palpable subcutaneous bone fragment
- indicates proximal fragment buttonholed through brachialis
- implies more serious injury, higher likelihood of arterial injury, significant swelling, more difficult closed reduction
- "floating elbow"
- ipsilateral supracondylar humerus and forearm/wrist fractures warrant timely pinning of both fractures to decrease the risk of compartment syndrome
- technique
- check vascular status after reduction
- if evidence of good distal perfusion admit for 48 hours of observation
- if not well perfused perform vascular exploration
- emergent (within hours)
- indications
- pulseless, poorly perfused hand
- technique
- check vascular status after reduction
- if well perfused admit and observe for 48 hours
- if not well perfused perform vascular exploration
- emergent vascular exploration and CRPP
- indications
- pulseless white hand (pale, cool, no doppler) following CRPP
- pulsatile and perfused hand that loses pulse following CRPP
- technique
- remove K-wires and reassess vascular status
- open exploration and reduction if vascular status does not improve
- open reduction, percutaneous pinning, +/- vascular exploration
- indications
- failed closed reduction
- more frequently required with flexion type fractures (compared to extension type)
- pulseless white OR pink hand that is unable to be reduced or there remains a gap
- gap might represent entrapped vascular structure
|
| Techniques |
- Closed reduction and percutaneous pinning (CRPP)
- fixation
- closed reduction (extension-type)
- posteromedial displacement: forearm pronated with hyperflexion
- posterolateral displacement: forearm supinated with hyperflexion
- if pronation or supination does not work, try the opposite
- 2 lateral pins
- usually sufficient in type II fractures
- test stability under fluoroscopy
- technical pearls
- maximize separation of pins at fracture site
- engage both medial & lateral columns proximal to fracture
- engage sufficient bone in proximal & distal segments
- low threshold for 3rd lateral pin if concern about stability with first 2 pins
- 3 lateral pins
- biomechanically stronger in bending and torsion than 2-pin constructs
- indications (where 2 lateral pins are insufficient)
- comminution
- type III and type IV (free floating distal fragment)
- no significant difference in stability between three lateral pins and crossed pins
- risk of iatrogenic nerve injury from a medial pin makes three lateral pins the construct of choice
- crossed pins
- biomechanically strongest to torsional stress
- higher risk of ulnar nerve injury (3-8%)
- highest risk if placed with elbow in hyperflexion as ulnar nerve subluxates anteriorly over medial epicondyle in some children
- reduce the risk of ulnar nerve injury by
- placing medial pin with elbow in extension
- use small medial incision (rather than percutaneous pinning)
- remove pins postop at 3 weeks
- Open Reduction with Percutaneous Pinning
- approach
- anterior approach if pulseless or median nerve injury
- a lateral or medial approach where periosteum is torn
- never posterior as posterior dissection can --> AVN
- soft tissue
- identify median nerve and brachial artery
- bone work
- confirm reduction with C-arm
- instrumentation
- 2 or 3 K-wires depending on the degree of stability
|
| Complications |
- Pin migration
- most common complication (~2%)
- Infection
- occurs in 1-2.4%
- typically superficial and treated with oral antibiotics
- Cubitus valgus
- caused by fracture malunion
- can lead to tardy ulnar nerve palsy
- Cubitus varus (gunstock deformity)
- caused by fracture varus malunion, especially in medial comminution pattern

- is NOT caused by growth disturbance
- usually a cosmetic issue with little functional limitations, but may be present
- Recurvatum
- common with non-operative treatment of Type II and Type III fractures
- Nerve palsy from injury
- usually resolve, nerves rarely torn
- extension type fractures
- neuropraxia in 11%
- most commonly AIN
- mechanism = tenting of nerve on fracture, or entrapment in the fracture site
- flexion type fractures
- neuropraxia in 17%
- most commonly cause ulnar neuropraxia
- Vascular Injury
- radial pulse absent on initial presentation in 7-12%
- pulseless hand after closed reduction and pinning (3-4%)
- decision to explore is based on quality of extremity perfusion rather than absence of pulse
- arteriography is NOT indicated in isolated injuries
- role of doppler is unclear and does not change treatment
- Volkmann ischemic contracture
- rare, but dreaded complication
- may result from elbow hyperflexion casting
- increase in deep volar forearm compartment pressures and loss of radial pulse with elbow flexed >90°
- rarely seen with CRPP and postoperative immobilization in less than 90°
- Postoperative stiffness
- rare after casting or after pinning procedures
- remove pins and allow gentle ROM at 3-4 weeks postop
- resolves by 6 months
- literature does not support the use of physical therapy
|