

Journal of American Science 2015;11(9) http://www.jofamericanscience.org
39
Characteristics of ischemic stroke in asymptomatic hepatitis C virus positive patients
Gharib Fawi 1, Hazem K. Elhewag 1
, Hassan M Elnady 1
, Al-Amir Bassiony Mohamed 1
, Ahmed Ezzat 1
, Hesham M
Hefny2
, Mahmoud Saif-Al Islam 3
, Mohamad H Alam-Eldeen 4
1
Department of Neurology, Faculty of Medicine, Sohag University, Egypt. 2
Department of Clinical Pathology, Faculty of Medicine, Sohag University, Egypt.
3
Department of Tropical Medicine and Gastroenterology, Faculty of Medicine, Sohag University, Egypt. 4
Department of Diagnostic Radiology, Faculty of Medicine, Sohag University, Egypt.
elnadyhassan1974@hotmail.com
Abstract: Background and aim of the study: Cerebrovascular diseases are leading cause of death worldwide.
Acute ischemic cerebrovascular events, including ischemic stroke (IS) , transient ischemic attack, and lacunar
syndromes, have been reported in hepatitis C virus infected patients. Various surveys were designed to study the
associations and pathophysiology of ischemic stroke in patients with hepatitis C virus infected patients. The purpose
of our work was to determine the Characteristics of ischemic stroke in hepatitis C virus infected patients. Patients
and Methods: Forty ischemic stroke patients with positive hepatitis C virus antibodies compared with 20 ischemic
stroke patients with negative hepatitis C virus antibodies. We examined traditional vascular risk factors, stroke
severity, carotid atherosclerosis, and a range of radiological and laboratory markers. The results: IS patients with
positive hepatitis C virus (HCV) antibodies were significantly younger (62.8±7.7, versus 67.3±7, P= 0.007). The
risk of stroke recurrence is significantly higher in ischemic stroke with positive HCV antibodies (32.2% versus 5%,
P=0.028), with larger numbers (P=0.026) but smaller sizes (4.544 cm3 versus 17.492 cm3, P=0.007) in addition to
significantly higher association with carotid atherosclerosis (73.3% versus 28.5%., P=0.047) and less severe stroke
(P=0.028) than those with negative hepatitis C virus antibodies. Conclusion: Our results show that hepatitis C virus
infection can accelerate atherosclerosis and leading to stroke at a relatively younger age with increased incidence of
stroke recurrence and usually associated with small lacunar syndromes and less severe stroke.
[Fawi G, Elhewag HK, Elnady HM, Mohamed AB, Ezzat A, Hefny HM, Saif-Al Islam M, Alam-Eldeen MH.
Characteristics of ischemic stroke in asymptomatic hepatitis C virus positive patients. J Am Sci 2015;11(9):39-
44]. (ISSN: 1545-1003). http://www.jofamericanscience.org. 5
Keywords: HCV • Ischemic stroke • Atherosclerosis
Introduction
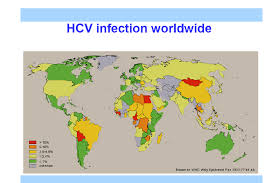
The worldwide prevalence of hepatitis C virus
(HCV) is to be 170 million individuals (1). Egypt
receives the highest prevalence of hepatitis C virus in
the world with more than 14.7% of the Egyptian
population have HCV infection (2).
In HCV infected patients , acute vascular events,
including ischemic stroke, transient ischemic attack,
and lacunar syndromes have been reported (3), these
ischemic events may be the presenting manifestation
of HCV infection in some cases (4).
Some factors may explain the associations and
pathophysiology of ischemic stroke in patients with
HCV infected patients. First the presence of
anticardiolipin antibodies may play an important role
in acute ischemic stroke (5). Second , hypertension
(6), type 2 DM is thought to be prevalent in chronic
HCV patients (7). Besides, it is well documented that
HCV infection, especially in those with elevated
hepatitis C viral load has a part in the development of
carotid atherosclerosis (8),(9). Finally HCV may be an
indirect risk factor of stroke by occlusive
vasculopathy and vasculitis which are well known in
HCV patients (10).
Aim of the work
The purpose of this work was to ascertain the
characteristics of ischemic stroke in HCV infected
patients.
Patients and methods
This is a comparative study, comparing ischemic
stroke patients with and without positive HCV
antibodies. We prospectively compared data from
consecutive ischemic stroke patients with (group A)
and without (group B) HCV antibodies. Patients in the
study were admitted to Department of Neurology,
Sohag University Hospital in the period between June
2013 and May 2014. Stroke was defined according to
the definition of the World Health Organization as the
rapid onset of a new persistent neurological deficit
attributable to an obstruction in cerebral blood flow
with no apparent non-vascular cause (11). The work
was approved by the Medical Research, Ethical
Committee of Sohag Faculty of Medicine. All
participants signed written consents. Patients were
excluded from the study if they had a hemorrhagic
stroke, transient ischemic attack (TIA), previous
diagnosis and/or current ischemic heart disease,
Journal of American Science 2015;11(9) http://www.jofamericanscience.org
40
cardiac valvular disease, congestive heart failure,
cardiomyopathies, and advanced renal or liver disease.
All patients were subjected to full history taking,
complete medical and neurological exam. Patients
with past or current history of smoking were
categorized as smokers. Hypertension was defined as
self-report of hypertension with antihypertensive
medication use, and/or systolic blood pressure greater
than or equal to 140 mm Hg, and/or diastolic blood
pressure greater than or equal to 90 mm Hg. Diabetes
was defined as being on treatment for diabetes by selfreport
and/or having a fasting glucose level greater
than or equal to 126 mg/dL. Hypercholesterolemia
was defined as a cholesterol level of more than 200
mg/dL or in the presence of a specific treatment.
Hypertriglyceridemia was defined as a triglyceride
level of more than 200 mg/dL. Admission stroke
severity was assessed by the Scandinavian Stroke
Scale (SSS). The SSS is a validated neurological
stroke scale that evaluates stroke severity on a score
from 0 to 58, with lower scores indicating moresevere
strokes (12).
Approximately 10 ml venous blood was drawn
from each study included in this study by a clean
venipuncture under aseptic conditions and divided into
EDTA, sodium citrate 3.8% and plain vacutainer
tubes. The sera were separated by centrifugation after
clotting and were stored at - 20 °C until analyzed.
Biochemical assays for serum alanine
Aminotransferase (ALT), aspartate aminotransferase
(AST), total bilirubin (Bil. T), direct bilirubin (Bil. D),
albumin, cholesterol, triglyceride (TG) and creatinine
were determined by Cobas c311 Chemistry Analyzer
System (Roche Diagnostics, GmbH, Mannheim,
Germany). Erythrocyte sedimentation rate and
Complete Blood Count (CBC): CBC was done by
Cell-Dyn 3700 (Abbott Laboratories, Diagnostic
Division, IL, USA). Prothrombin time - INR was
studied with a Sysmex CA-1500 coagulometer
(Siemens, Healthcare Diagnostics Inc, USA).
Serological testing for both anti-HCV and HBsAg
were evaluated by the Architect i1000SR system
(Abbott Laboratories, Diagnostics Division, IL, USA).
CT brain was done for all patients to evaluate the
site and size of ischemic lesion. The size of the lesion
was measured according to radiological parameters.
The size was detected by the largest diameter (A) of
the infarct and its largest perpendicular diameter (B)
was measured. The third, vertical diameter (C) was
determined by summation the thicknesses of the slices
in which the lesion was visible. Infarct volume was
calculated according to the formula: Size = 0.5x A x B
x C (13). Echocardiography was performed for all
patients. Carotid Doppler was done by high-resolution
B-mode ultrasonography equipped with a 7.5 MHz
linear-array transducer. Extracranial carotid arteries
were scanned bilaterally along the anterior, lateral,
and posterior axes, in transverse and longitudinal
planes. Patients were lying in a supine position with
the neck was in mild Hyperextension position as well
as almost 45 degree rotation away from the examined
side. Measurements were taken in on frozen images of
carotid arteries at the level of the common carotid
arteries, internal carotid arteries and bulb tracts. On
the screen displaying the frozen image, 2 cursors were
positioned on the boundaries of the intima and media
respectively. The distance between the cursors was
recorded to the nearest 0.1 mm. Intima-media
thickness (IMT) of the common carotid arteries was
considered as the distance between the lumen-intima
interface and the leading edge of media-adventitia
interface (14). Thus, only the intima which appears as
echogenic layer and the media which appears as echopoor
layer were included in the measurement (15).
IMT measurements of the carotid artery were taken in
triplicate for each site and the mean value was
calculated and recorded. In agreement with the
Mannheim Carotid Intima-Media Thickness
Consensus, IMT >1 mm was regarded as a cut-off
value for carotid atherosclerosis (CA) given that it is
associated with a 3-4 fold increased risk of subsequent
ischemic stroke (16). Plaques were defined as
protrusions into the vessel lumen of at least 1.5 mm,
as assessed from the boundary line between the
adventitial and median layers. The term "CA" was
applied to show the overall occurrence, e.g., increased
IMT (>1 mm) and /or plaques.
Statistical data analysis:
The data were analyzed by Statistical Package
for the Social Sciences (SPSS version 20) for
windows. Continuous data were expressed as mean ±
SD, and categorical data were expressed as numbers
and percent. Comparisons of differences between two
groups were executed by the Student's t-test for the
continuous data, Chi-square test for categorical data. P
values equal or less than 0.05 were considered
statistically significant.
Results:
During the period of the study, the inclusion
criteria were applied on 60 ischemic stroke (IS)
patients (30 males and 30 females). Forty patients
were categorized as group A and 20 patients as group
B. The characteristics of the 60 subjects included in
the study are reported in Table 1. Our results showed
that the IS patients with positive HCV antibodies
(group A) were significantly younger than those with
negative HCV antibodies (group B). The mean age of
the first group was 62.8±7.7, while in group B was
67.3±7 (P = 0.007). No sex difference was reported
between the 2 groups. Smoking was non significntly
more prevalent in group A than in group B (P=0. 1).
Journal of American Science 2015;11(9) http://www.jofamericanscience.org
41
Stroke recurrence was significantly higher in group A
(P = 0.028). No significant differences were detected
between both groups regarding the prevalence of
diabetes mellitus or hypertension. Stroke severity,
measured by SSS, was significantly higher in patients
with negative HCV antibodies (P=0.028). Carotid
atherosclerosis was significantly more prevalent
among group A patients (p = 0.047) (Figure 1). Stroke
patients with HCV antibodies had significantly higher
number, but smaller sizes of brain ischemic lesions (p
= 0.003, p = 0.047 respectively) (Table 2). Stroke
patients with HCV infection showed significantly
higher serum levels of total serum bilirubin (P=0.048),
direct bilirubin (P=0.034), ALT (P=0.009), AST
(P=0.040), triglycerides (P=0.010) and ESR (P=0.020)
than those without CV infection (Table 3).
Discussion:
This study revealed that stroke patients with
positive HCV antibodies were significantly younger,
carry higher risk of recurrence, with larger numbers
but smaller sizes of ischemic lesions, with
significantly higher association with CA and less
severe stroke than those with negative HCV
antibodies. In a large prospective population-based
cohort, Liao and colleagues (17) demonstrated that the
cumulative risk of stroke is significantly higher for
HCV positive subjects. Similarly , a communitybased
prospective cohort study reported that chronic
HCV infection with increasing serum HCV RNA level
is not only a predictor of stroke severeity but also an
independent risk predictor of stroke deaths (18).
Adinolfi and colleagues (19) reported that the
prevalence of HCV infection in stroke patients is
significantly higher and this finding coupled with
those reported by others(17, 18) complete the HCVstroke
puzzle (high prevalence, incidence and
mortality) that strongly suggests a strict association
between chronic HCV infection and stroke event.
Table 1. Characteristics at the admission of the 60
patients included in the study
Group A
IS with HCV +ve
antibodies
Group B
IS with HCV ̶ve
antibodies
Pvalue
Number of
cases 40 20
Age, M±SD 62.8 ±7.7 67.3± 4.6 0.007
Males no.(%) 22 (55%) 8 (40%) 0.44
Smoking 12 (30%) 5 (25%) 0.1
DM 17 (42.5%) 7 (35%) 0.5
Hypertension 30 (75%) 13 (65%) 0.4
Previous CVS 13 (32.5%) 1(5%) 0.028
SSS 38.2 ± 13.26 25.3 ± 17.2 0.028
IS: ischemic stroke, HCV: hepatitis C virus, DM: diabetes
mellitus, CVS: cerebrovascular stroke, SSS: Scandinavian
Stroke Scale
Figure (1): Percentage of patients with carotid
atherosclerosis in both groups.
Table 2: Radiological characters of ischemic lesions in
both groups
Group A Group B Total P value
Number of
lesions
1 26 20 46 0.026 >1 14 0 14
Total 40 20 60
Mean size of
infarction
4.544
cm3
17.492
cm3 0.007
HCV: hepatitis C virus
Table (3): Laboratory findings in both groups
Group A Group B P value Mean SD Mean SD
Total bilirubin 1.11 0.755 0.745 0.394 0.048
Direct bilirubin 0.587 0.512 0.336 0.202 0.034
ALT 45.775 33.801 39.85 9.298 0.009
AST 47.425 34.254 37.75 12.628 0.040
Albumin 3.269 0.707 3.48 0.726 0.173
Cholesterol 180.675 59.692 184.95 61.659 0.813
Triglycerides 205.65 105.566 167.75 62.08 0.010
Platelets 221.32 116.416 175.075 50.35 0.094
Creatinine 1.295 1.317 2.08 2.375 0.053
WBCs 9.258 3.795 7.537 3.349 0.134
PT 13.154 1.818 13.15 1.312 0.255
PC 82.108 14.663 83.45 11.814 0.513
INR 1.1605 0.152 1.159 0.169 0.315
ESR 36.50 30.31 15.8 16.694 0.020
ALT: alanine transaminase, AST: aspartate transaminase,
PT: prothrombin time, PC: prothrombin concentration,
ESR: erythrocytic sedimentation rate, WBCs: white blood
cells, INR: international normalization ratio
The present work revealed that stroke patients
with HCV were significantly younger than those
without. This is in accord with a study by Adinolfi and
colleagues who reported that HCV is a hazard element
for an earlier stroke. It is important to underline that
such ischemic event occurs despite HCV infected
patients showed a more favorable risk profile such as
lower lipid levels, lower prevalence of hypertension
and of the male sex; in addition, the ischemic event in
0.00%
20.00%
40.00%
60.00%
80.00%
stroke without stroke with CHC
CHC
Percentage of patients with
carotid atherosclerosis
Journal of American Science 2015;11(9) http://www.jofamericanscience.org
42
anti-HCV positive patients occurs in younger age than
those with anti-HCV negative. The data strongly
support a direct role of HCV in determining
conditions that favor ischemic cerebral events (19).
Stroke recurrence, in our study, was more
common in patients with positive HCV antibodies. We
found that the history of previous ischemic stroke was
significantly higher in those with positive HCV
antibodies than those without (P=0.015). This data
from patients history is enforced by brain CT findings,
which showed significantly higher number of previous
cerebral infarctions in patients with positive HCV
antibodies than those without (P = 0.026). This is in
agreement with Fuckar and colleagues (6) and Lee and
colleagues (18) who concluded that HCV is a risk
factor for stroke recurrence. The authors of these
previous studies reported that, this may be due to
enhancement of the effect of other risk factors like
hypertension or directly by the vasculitic changes of
small brain vessels associated with HCV infection(6,
18).
In our study, we found that stroke patients with
positive HCV antibodies showed significantly higher
serum triglycerides (p = 0.006), and insignificantly
lower serum cholesterol (p = 0.8) when compared to
stroke patients with negative HCV antibodies. In
2001, Serfaty (20) reported that serum cholesterol
concentration was significantly lower in HCV patients
than in controls. Another study (21) has shown that
patients with HCV-3 infection have age-adjusted
hypocholesterolemia and more frequent hepatic
steatosis. Moreover, Adinolfi and colleagues (22) and
Butt and colleagues (23) reported that stroke patients
with CHC had lower levels of cholesterol. The extent
of liver steatosis is inversely related to the serum
cholesterol concentrations, which suggests that a
common pathway may underlie this metabolic
disturbance (24, 25). In a Japanese study,(26)
infection by HCV genotype-1b also induced a higher
degree of hypocholesterolemia and
hypobetalipoproteinaemia than HBV infection. The
cause of this interaction is unknown, but the lowdensity
lipoprotein receptors have been proposed as
the recognition receptor for HCV entry in hepatocytes
(27, 28).
One of the most important findings in the current
study was an increased prevalence of carotid
atherosclerosis in stroke patients with positive HCV
antibodies than those without. This data agrees with
the findings of previous studies (29-32), the largest
one of them showing that HCV infected subjects had a
significant higher prevalence of atherosclerosis
despite being younger and having a more favorable
cardiovascular risk profile (23). In 2012, Adinolfi and
colleagues (22) reported that CHC patients had a
significantly higher prevalence of CA compared with
a matched control population (53.7% vs 34.3%).
Furthermore, amongst the younger CHC patients (e.g.
<50 years old) about 34% showed CA versus (16.0%)
in the control group and a significant proportion
(24.1%) had plaques, which was a rare event in the
control group (3.9%). Their data supported the view
that chronic HCV infection predisposes prematurely to
the development of CA and of advanced lesions
despite the more favorable cardiovascular risk profile
featuring lower lipid levels, lower prevalence of
metabolic syndrome and possible a lower prevalence
of hypertension (33).
Several previous findings contributed to advance
the understanding of pathogenic mechanisms linking
HCV infection with early and advanced
atherosclerosis. Serum HCV RNA levels were found
to be independently associated with CA, in particular
with both early phases of IMT lesion and advanced
phase of plaques (22). In 2010, HCV RNA sequences
were isolated inside carotid plaques and it was
indicated that HCV replicates within CA (9). Taken
together, these findings support a direct proatherogenic
action of HCV, which could contribute
per se to premature arterial ageing (9). An interesting
previous finding is the demonstration that HCV
patients with steatosis, irrespective of HCV genotype,
age, gender and degree of histological liver damage,
carried the highest prevalence of atherosclerosis
(77.7%) (22). Moreover, HCV-related steatosis was an
independent risk factor for atherosclerosis. HCV
related steatosis has a good predictive ability to
atherosclerosis with a good specificity and sensitivity
(22).
The significantly higher serum triglycerides
among HCV positive stroke patients, found in our
study, could explain the increased prevalence of
carotid atherosclerosis in this group. This is in
agreement with Adinolfi and colleagues (22) who
reported that higher levels of serum triglycerides and
not serum cholesterol were significantly associated
with carotid atherosclerosis in CHC patients.
The data of the present study show that HCV
patients with stroke had had a significant higher level
of ESR. These data strongly support the hypothesis
that chronic HCV infection increases the risk of
ischemic stroke through higher systemic inflammatory
levels (19). It is evident that the instability of
atheromatous plaque is at the base of ischemic events.
It is also well known that inflammation play a major
role in the instability of plaque (34). It has been
suggested that infectious agents may induce
atherosclerosis by inflammatory stimuli either locally
within vascular wall or systemically through
inflammatory mediators (35).
In this context, it has been demonstrated that
HCV lives and replicates within carotid plaque (9) and
Journal of American Science 2015;11(9) http://www.jofamericanscience.org
43
the virus enters and replicates inside human brain
endothelial cells (36). Moreover, it has been
demonstrated that HCV infection is associated with
atherosclerosis by increasing local and systemic
inflammation (37-39).
Adinolfi and colleagues (19) reported that HCV
patients with stroke had significantly higher serum
levels of inflammatory markers than negative ones; in
particular HCV positive patients had significant higher
levels of ESR, CRP and serum fibrinogen.
They also reported that, considering that HCV
replicate within endothelial cells and within plaque, it
is likely that in HCV infection a local inflammation of
vascular endothelia and/or within plaque may occur.
Such chronic inflammatory condition could promote
not only the development of atheromas, but also its
destabilization and, therefore, a higher risk of
occlusive or embolic stenosis (19).
The present study revealed that the stroke
severity was significantly lower in patients with
positive HCV antibodies. In agreement with previous
studies, HCV is more likely to cause small vessel
disease and lacunar infarctions by its vasculitic
changes on small brain vessels (3, 6).
Conclusion:
Our results show that HCV infection can
accelerate atherosclerosis and leading to to stroke at a
relatively younger age, with increase incidence of
stroke recurrence and usually associated with small
lacunas and less severe stroke.
Corresponding Author:
Hassan M Elnady
Faculty of medicine
Department of Neurology, Sohag University, Egypt.
E-mail: elnadyhassan1974@hotmail.com
References
1. Khattab MA. Targeting host factors: a novel rationale
for the management of hepatitis C virus. World journal
of gastroenterology : WJG. 2009;15(28):3472-9.
2. Cuadros DF, Branscum AJ, Miller FD, Abu-Raddad
LJ. Spatial epidemiology of hepatitis C virus infection
in Egypt: analyses and implications. Hepatology.
2014;60(4):1150-9.
3. Origgi L, Vanoli M, Carbone A, Grasso M, Scorza R.
Central nervous system involvement in patients with
HCV-related cryoglobulinemia. The American journal
of the medical sciences. 1998;315(3):208-10.
4. Cacoub P, Raguin G, Veyssier P, Piette JC, Micoud
M, Godeau P. [Hepatitis C virus infection in internal
medicine and infectious diseases departments in
France. Preliminary results of a national
epidemiological survey]. Presse Med. 1996;25(8):349-
52.
5. Cojocaru IM, Cojocaru M, Iacob SA, Burcin C.
Cerebral ischemic attack secondary to hepatitis C virus
infection. Romanian journal of internal medicine =
Revue roumaine de medecine interne. 2005;43(3-
4):255-60.
6. Fuckar K, Lakusic N, Mahovic D, Hirs I. Recurrent
strokes as a leading presentation of chronic hepatitis C
infection. Archives of medical research.
2008;39(3):358-9.
7. Allison ME, Wreghitt T, Palmer CR, Alexander GJ.
Evidence for a link between hepatitis C virus infection
and diabetes mellitus in a cirrhotic population. Journal
of hepatology. 1994;21(6):1135-9.
8. Wang CH, Chen CJ, Lee MH, Yang HI, Hsiao CK.
Chronic hepatitis B infection and risk of
atherosclerosis-related mortality: A 17-year follow-up
study based on 22,472 residents in Taiwan.
Atherosclerosis. 2010;211(2):624-9.
9. Boddi M, Abbate R, Chellini B, Giusti B, Giannini C,
Pratesi G, et al. Hepatitis C virus RNA localization in
human carotid plaques. Journal of clinical virology :
the official publication of the Pan American Society
for Clinical Virology. 2010;47(1):72-5.
10. Heckmann JG, Kayser C, Heuss D, Manger B, Blum
HE, Neundorfer B. Neurological manifestations of
chronic hepatitis C. Journal of neurology.
1999;246(6):486-91.
11. Hatano S. Experience from a multicentre stroke
register: a preliminary report. Bulletin of the World
Health Organization. 1976;54(5):541-53.
12. Barber M, Fail M, Shields M, Stott DJ, Langhorne P.
Validity and reliability of estimating the scandinavian
stroke scale score from medical records. Cerebrovasc
Dis. 2004;17(2-3):224-7.
13. Pantano P, Caramia F, Bozzao L, Dieler C, von
Kummer R. Delayed increase in infarct volume after
cerebral ischemia: correlations with thrombolytic
treatment and clinical outcome. Stroke; a journal of
cerebral circulation. 1999;30(3):502-7.
14. Allan PL, Mowbray PI, Lee AJ, Fowkes FG.
Relationship between carotid intima-media thickness
and symptomatic and asymptomatic peripheral arterial
disease. The Edinburgh Artery Study. Stroke; a journal
of cerebral circulation. 1997;28(2):348-53.
15. Tahmasebpour HR, Buckley AR, Cooperberg PL, Fix
CH. Sonographic examination of the carotid arteries.
Radiographics: a review publication of the
Radiological Society of North America, Inc.
2005;25(6):1561-75.
16. Touboul PJ, Hennerici MG, Meairs S, Adams H,
Amarenco P, Bornstein N, et al. Mannheim carotid
intima-media thickness consensus (2004-2006). An
update on behalf of the Advisory Board of the 3rd and
4th Watching the Risk Symposium, 13th and 15th
European Stroke Conferences, Mannheim, Germany,
2004, and Brussels, Belgium, 2006. Cerebrovasc Dis.
2007;23(1):75-80.
17. Liao CC, Su TC, Sung FC, Chou WH, Chen TL. Does
hepatitis C virus infection increase risk for stroke? A
population-based cohort study. PloS one.
2012;7(2):e31527.
18. Lee MH, Yang HI, Wang CH, Jen CL, Yeh SH, Liu
CJ, et al. Hepatitis C virus infection and increased risk
Journal of American Science 2015;11(9) http://www.jofamericanscience.org
44
of cerebrovascular disease. Stroke; a journal of
cerebral circulation. 2010;41(12):2894-900.
19. Adinolfi LE, Restivo L, Guerrera B, Sellitto A, Ciervo
A, Iuliano N, et al. Chronic HCV infection is a risk
factor of ischemic stroke. Atherosclerosis.
2013;231(1):22-6.
20. Serfaty L, Andreani T, Giral P, Carbonell N,
Chazouilleres O, Poupon R. Hepatitis C virus induced
hypobetalipoproteinemia: a possible mechanism for
steatosis in chronic hepatitis C. Journal of hepatology.
2001;34(3):428-34.
21. Fernandez-Rodriguez CM, Lopez-Serrano P, Alonso
S, Gutierrez ML, Lledo JL, Perez-Calle JL, et al.
Long-term reversal of hypocholesterolaemia in
patients with chronic hepatitis C is related to sustained
viral response and viral genotype. Alimentary
pharmacology & therapeutics. 2006;24(3):507-12.
22. Adinolfi LE, Restivo L, Zampino R, Guerrera B,
Lonardo A, Ruggiero L, et al. Chronic HCV infection
is a risk of atherosclerosis. Role of HCV and HCVrelated
steatosis. Atherosclerosis. 2012;221(2):496-
502.
23. Butt AA, Xiaoqiang W, Budoff M, Leaf D, Kuller LH,
Justice AC. Hepatitis C virus infection and the risk of
coronary disease. Clinical infectious diseases : an
official publication of the Infectious Diseases Society
of America. 2009;49(2):225-32.
24. Hofer H, Bankl HC, Wrba F, Steindl-Munda P, PeckRadosavljevic
M, Osterreicher C, et al. Hepatocellular
fat accumulation and low serum cholesterol in patients
infected with HCV-3a. The American journal of
gastroenterology. 2002;97(11):2880-5.
25. Poynard T, Ratziu V, McHutchison J, Manns M,
Goodman Z, Zeuzem S, et al. Effect of treatment with
peginterferon or interferon alfa-2b and ribavirin on
steatosis in patients infected with hepatitis C.
Hepatology. 2003;38(1):75-85.
26. Moriya K, Shintani Y, Fujie H, Miyoshi H, Tsutsumi
T, Yotsuyanagi H, et al. Serum lipid profile of patients
with genotype 1b hepatitis C viral infection in Japan.
Hepatology research : the official journal of the Japan
Society of Hepatology. 2003;25(4):371-6.
27. Monazahian M, Bohme I, Bonk S, Koch A, Scholz C,
Grethe S, et al. Low density lipoprotein receptor as a
candidate receptor for hepatitis C virus. Journal of
medical virology. 1999;57(3):223-9.
28. Agnello V, Abel G, Elfahal M, Knight GB, Zhang
QX. Hepatitis C virus and other flaviviridae viruses
enter cells via low density lipoprotein receptor.
Proceedings of the National Academy of Sciences of
the United States of America. 1999;96(22):12766-71.
29. Ishizaka N, Ishizaka Y, Takahashi E, Tooda E,
Hashimoto H, Nagai R, et al. Association between
hepatitis C virus seropositivity, carotid-artery plaque,
and intima-media thickening. Lancet.
2002;359(9301):133-5.
30. Ishizaka Y, Ishizaka N, Takahashi E, Unuma T, Tooda
E, Hashimoto H, et al. Association between hepatitis C
virus core protein and carotid atherosclerosis.
Circulation journal : official journal of the Japanese
Circulation Society. 2003;67(1):26-30.
31. Vassalle C, Masini S, Bianchi F, Zucchelli GC.
Evidence for association between hepatitis C virus
seropositivity and coronary artery disease. Heart.
2004;90(5):565-6.
32. Targher G, Bertolini L, Padovani R, Rodella S, Arcaro
G, Day C. Differences and similarities in early
atherosclerosis between patients with non-alcoholic
steatohepatitis and chronic hepatitis B and C. Journal
of hepatology. 2007;46(6):1126-32.
33. Adinolfi LE, Restivo L, Zampino R, Lonardo A, Loria
P. Metabolic alterations and chronic hepatitis C:
treatment strategies. Expert opinion on
pharmacotherapy. 2011;12(14):2215-34. 34.
34. Libby P. Inflammation in atherosclerosis. Nature.
2002;420(6917):868-74.
35. Hansson GK. Inflammation, atherosclerosis, and
coronary artery disease. The New England journal of
medicine. 2005;352(16):1685-95.
36. Fletcher NF, Wilson GK, Murray J, Hu K, Lewis A,
Reynolds GM, et al. Hepatitis C virus infects the
endothelial cells of the blood-brain barrier.
Gastroenterology. 2012;142(3):634-43 e6.
37. Lonardo A, Lombardini S, Scaglioni F, Carulli L,
Ricchi M, Ganazzi D, et al. Hepatic steatosis and
insulin resistance: does etiology make a difference?
Journal of hepatology. 2006;44(1):190-6. 38.
38. Vivona N, Bivona G, Noto D, Sasso BL, Cefalu AB,
Chiarello G, et al. C-reactive protein but not soluble
CD40 ligand and homocysteine is associated to
common atherosclerotic risk factors in a cohort of
coronary artery disease patients. Clinical biochemistry.
2009;42(16-17):1713-8.
39. Oliveira CP, Kappel CR, Siqueira ER, Lima VM,
Stefano JT, Michalczuk MT, et al. Effects of hepatitis
C virus on cardiovascular risk in infected patients: a
comparative study. International journal of cardiology.
2013;164(2):221-6.
8/16/2015