

Background
The management of CAF at a time shifted from surgical to medical treatment; chemical sphincterotomy through nitric oxide (NO) donors, calcium-channel blockers or botulinum toxin combined with stool softeners and life-style changes. In resistant CAF, the surgical choice is necessary. Lateral internal sphincterotomy (LIS) has long been the gold standard. Its early results have been favourable, but there is concern over continence in the long term after LIS. Fissurectomy with or without anoplasty, described in our study is an alternative with no or minimal effect on anal continence.
Aim of the work: This study purpose is to assess the safety and short-term outcome results of fissurectomy with or without anoplasty (simple cutaneous advancement flap) as a sphincter saving surgical technique in chronic anal fissure (CAF) and to compare between both procedures regarding post-operative patient's satisfaction, complications and wound healing.
Method: Thirty-Seven series of patients (18 females), who had undergone fissurectomy with anal dilatation alone (14 patients) or combined with anoplasty (23 patients) for a medically resistant CAF, who were admitted at Sohag university hospitals from July 2016 were included in the study. At a duration of follow-up of 6 months, regular outpatient clinic visits for all patients; assessing postoperative pain (on visual analogue scale), wound healing, recurrence, satisfaction with the operation and faecal continence (on Pescatori score).
Statistical analysis:
Data were recorded using Microsoft Excel 2010 program (Microsoft Co, USA). Normality of data distribution was checked by Shapiro Wilk test. The box plots were used to identify and exclude outliers.
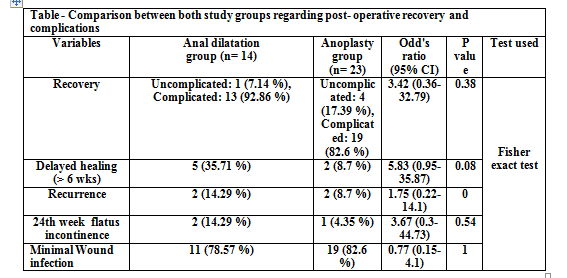
Results: The mean age was 39.9(SD ±11.95) years. Thirty-two cases (86.4%) were presented at admission with anal pain. Duration of anal fissure ranges from (4-18) months.Five patients had a recurrent CAF (11.6%). Twenty-four cases (64.8%) had posterior anal fissure. Healing time ranged from 6-12 weeks (mean 9 weeks). First day postoperative pain score ranges from 2-7 degrees and managed by simple analgesics. The 6th week pain score ranges from 0-2 degrees for both groups. After complete healing and following soft diet instructions pain improved significantly. Recurrence occurs in 4 cases (10.8%) of a total 37 cases. All recurrence cases improved significantly conservatively by local care and good dietary habits. No reported incontinence to stool at all cases. Thirty cases were satisfied (81.1%) with the procedure.
Conclusion: Given its high rate of healing no effect on anal continence, fissurectomy with or without advancement flap for patients with CAF represents a safe, simple and valid sphincter saving procedure to manage resistant CAF successfully.