| Introduction |
- Infection of bone characterized by progressive inflammatory destruction and apposition of new bone
-
Epidemiology
-
risk factors
- recent trauma or surgery
- immunocompromised patients
- illicit IV drug use
- poor vascular supply
- systemic conditions such as diabetes and sickle cell
- peripheral neuropathy
-
Pathophysiology
-
mechanism of spread
-
hematogenous
- originated or transported by blood
- etiology of 20% of osteomyelitis
- vertebrae most common site
- S. aureus is most common organism
-
contiguous-focus
- associated with previous surgery, trauma, wounds, or poor vascularity
- can be bacterial (most common), mycobacterial, or fungal in nature
-
direct-inoculation
- penetrating injuries
- surgical contamination
-
biofilm formation
- bacteria produce biofilm that covers necrotic bone and hardware
- made of an extracellular polymeric substance or exopolysaccharide
- antibiotics have difficulty penetrating biofilm
-
organism
- organism varies by age of patient
- S. aureus is most common in adults
|
| Osteomyelitis Organism Table |
| Age group |
Most common organisms |
Newborns
(younger than 4 mo) |
S. aureus, Enterobacter species, and group A and B Streptococcus species |
Children
(aged 4 mo to 4 y) |
S. aureus, group A Streptococcus species, Kingella kingae, and Enterobacter species |
Children, adolescents
(aged 4 y to adult) |
S. aureus (80%), group A Streptococcus species, H. influenzae, and Enterobacter species |
| Adult |
S. aureus and occasionally Enterobacter or Streptococcus species |
| Sickle Cell Anemia Patients |
S. aureus is typically most common, but Salmonella species is pathognomonic |
|
-
Prognosis
-
philosophy of treatment
- infection elimination
- bone union
- despite surgical debridement and long-term antibiotics, recurrence rate of chronic osteomyelitis in adults is 30%
|
| Classification |
-
Timing classification
-
acute
-
subacute
- within one to several months
-
chronic
- Cierny classification
|
Cierny Classification of Osteomyelitis 
(describes anatomic involvement, host, treatment, prognosis) |
| Anatomic Location |
| Stage I |
Medullary |
  |
| Stage 2 |
Superficial |
|
| Stage 3 |
Localized |
|
| Stage 4 |
Diffuse |
|
| Host Type |
| Type A |
Normal |
|
| Type B |
Compromised |
|
| Type C |
Treatment is worse to patient than infection |
|
|
| |
| Presentation |
-
Symptoms
- pain
-
fever
- more common in acute osteomyelitis
-
Physical exam
- erythema, tenderness, and edema are commonly seen
- limp and/or pain inhibition with weight-bearing or motion may be present
-
draining sinus tract
- more common in chronic osteomyelitis
|
| Imaging |
-
Radiographs
-
recommended views
- orthogonal plain radiographs of the affected extremity
-
findings
- often shows a lytic region surrounded by an area of sclerosis
- may mimic a neoplastic processes
- bone loss must be 30-40% before evident on plain films
- sequestrum: devitalized bone that serves as a nidus for infection

- involucrum: formation of new bone around an area of bony necrosis
-
CT
- useful for surgical planning and determining extent of bony destruction
-
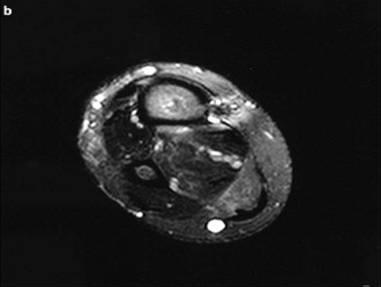
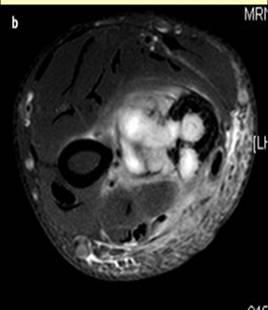
MRI
- useful for soft tissue evaluation
-
Bone Scan
- sensitivity comparable to MRI, but specificity is poor
|
| Studies |
-
Laboratory analysis
-
Microbiology
-
blood cultures
- may be used to guide therapy for hematogenous osteomyelitis
-
sinus tract cultures
- not reliable for guiding antibiotic therapy
-
bone biopsy
- gold-standard for guiding antibiotic therapy
|
| Treatment |
-
Goals
-
Nonoperative Treatment
-
Operative treatment
|
| Surgical Techniques |
-
Antibiotic therapy
-
technique
- antibiotics should be tailored to specific organism, preferably after a bone biopsy is obtained
- chronic suppressive antibiotics may be useful in patients who are immunocompromised or in whom surgery is not feasible
-
Irrigation & Debridement
-
technique
-
debridement
- all devitalized and necrotic tissue should be removed
- extensive debridement is essential to eradicate infection
- sequestrum must be eliminated from the body, or infection is likely to recur
-
hardware removal
- any non-essential hardware should be removed
-
dead space management
- goal is to replace dead bone and scar tissue with vascularized tissue
-
options include
- vascularized bone grafts
- local tissue flaps or free flaps
- antibiotic-impregnated acrylic beads (PMMA)
-
vacuum-assisted closure
-
stabilization
- bony stability is required for successful eradication of infection
- external fixation preferred to internal fixation
- mechanism is thought to be related to improved angiogenesis
|
| Complications |
- Persistence or extension of infection
- Amputation
- Sepsis
- Malignant transformation (Marjolin's ulcer)
|