| Introduction |
- "Both-bone" forearm fractures
- Epidemiology
- more common in men than women
- ratio of open to closed fractures is higher than for any other bone except tibia
- Mechanism
- direct trauma
- often while protecting one's head
- indirect trauma
- motor vehicle accidents
- falls from height
- athletic competition
- Associated conditions
- elbow injuries
- evaluate DRUJ and elbow for
- Galeazzi fractures

- Monteggia fractures
- compartment syndrome
- evaluate compartment pressures if concern for compartment syndrome
- Prognosis
- functional results depend on restoration of radial bow

|
| Anatomy |
- Osteology
- axis of rotation of forearm runs through radial head (proximal) and ulna fovea (distal)
- distal radius effectively rotates around the distal ulna in pronosupination
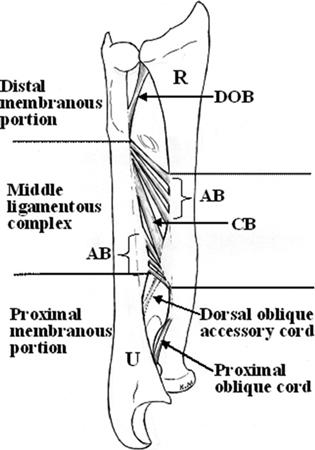
- Interosseous membrane (IOM)
- occupies the space between the radius and ulna
- comprised of 5 ligaments

- central band is key portion of IOM to be reconstructed
- accessory band
- distal oblique bundle
- proximal oblique cord
- dorsal oblique accessory cord
|
| Classification |
- Descriptive
- closed versus open
- location
- comminuted, segmental, multifragmented
- displacement
- angulation
- rotational alignment
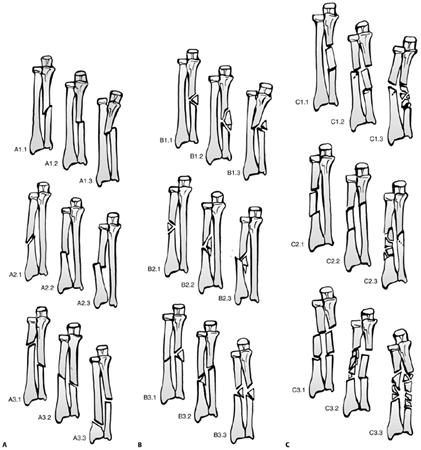
- OTA classification
- radial and ulna diaphyseal fractures
- Type A
- simple fracture of ulna (A1), radius (A2), or both bones (A3)
- Type B
- wedge fracture of ulna (B1), radius (B2), or both bones (B3)
- Type C
|
| Presentation |
- Symptoms
- gross deformity, pain, swelling
- loss of forearm and hand function
- Physical exam
- inspection
- open injuries
- check for tense forearm compartments
- neurovascular exam
- assess radial and ulnar pulses
- document median, radial, and ulnar nerve function
- pain with passive stretch of digits
- alert to impending or present compartment syndrome
|
| Imaging |
- Radiographs
- recommended views
- AP and lateral views of the forearm

- additional views
- oblique forearm views for further fracture definition
- ipsilateral wrist and elbow
- to evaluate for associated fractures or dislocation
- radial head must be aligned with the capitellum on all views
|
| Treatment |
- Nonoperative
- functional fx brace with good interosseous mold
- indications
- isolated nondisplaced or distal 2/3 ulna shaft fx (nightstick fx) with
- < 50% displacement and
- < 10° of angulation

- outcomes
- union rates > 96%
- acceptable to fix surgically due to long time to union
- Operative
- ORIF without bone grafting
- indications
- displaced distal 2/3 isolated ulna fxs
- proximal 1/3 isolated ulna fxs
- all radial shaft fxs (even if nondisplaced)
- both bone fxs
- Gustillo I, II, and IIIa open fractures may be treated with primary ORIF

- outcomes
- most important variable in functional outcome is to restore the radial bow
- ORIF with bone grafting
- indications
- cancellous autograft is indicated in radial and ulnar fractures with bone loss
- bone loss that is segmental or associated with open injury(delayed grafting in open injuries)
- nonunions of the forearm
- external fixation
- indications
- Gustillo IIIb and IIIc open fractures
- IM nailing
- indications
- poor soft-tissue integrity
- not preferred due to lack of rotational and axial stability and difficulty maintaining radial bow (higher nonunion rate)
|
| Techniques |
- ORIF
- approach
- usually performed through separate approaches due to risk of synostosis
- radius
- volar (Henry) approach to radius
- best for distal 1/3 and middle 1/3 radial fx
- dorsal (Thompson) approach to radius
- best for middle and proximal 1/3 radial fx
- ulna
- subcutaneous approach to ulna shaft
- technique
- 3.5 mm DCP plate (AO technique) is standard

- longer plates are preferred due to high torsional stress in forearm
- locked plates are increasingly indicated over conventional plates in osteoporotic bone and in bridging comminuted fractures
- bone grafting
- vascularized fibula grafts can be used for large defects and have a lower rate of infection
- postoperative care
- early ROM unless there is an injury to proximal or distal joint
- should be managed with a period of non-weight bearing due to risk of secondary displacement of the fracture
|
| Complications |
- Synostosis

- uncommon with an incidence of 3 to 9%
- associated with ORIF using a single incision approach
- heterotopic bone excision can be performed with low recurrence risk as early as 4-6 months post-injury when prophylactic radiation therapy and/or indomethacin are used postoperatively
- Infection
- Compartment syndrome
- increased risk with
- high energy crush injury
- open fxs
- low velocity GSWs
- vascular injuries
- coagulopathies (DIC)
- Nonunion
- commonly result from technical error or use of IM fixation
- atrophic nonunions can be treated with 3.5 mm plates and autogenous cancellous bone grafting
- Malunion
- direct correlation between restoration of radial bow and functional outcome
- Neurovascular injury
- uncommon except
- PIN injury with Monteggia fxs and Henry (volar) approach to middle and upper third radial diaphysis
- Type III open fxs
- observe for three months to see if nerve function returns
- explore if no return of function after 3 months
- Refracture
- increased risk with
- removing plate too early
- large plates (4.5 mm)
- comminuted fx
- persistent radiographic lucency
- do not remove plates before 15 mos.
- wear functional forearm brace for 6 weeks and protect activity for 3 mos. after plate removal
|