| Introduction |
- Progressive, pathologic genu varum centered at tibia
- Blount's disease is best divided into two distinct disease entities
- Infantile Blount's

- pathologic genu varum in children 0-3 years of age
- more common
- deformity rarely from femur
- typically affects both lower extremities
- Adolescent Blount's (this topic)
- pathologic genu varum in children > 10 years of age
- more likely to have femoral deformity
- less common
- less severe
- more likely to be unilateral
- Etiology
- Blount's is thought to be caused by a dyschondrosis of medial physis of proximal tibia
- likely multifactorial but related to mechanical overload in genetically susceptible individuals
- Risk factors
- obesity
- African-American descent
|
| |
Infantile Blounts |
Adolescent Blounts |
| Age |
2-5yrs |
>10yrs |
| Bilaterality |
50% bilateral |
Usually unilateral |
| Risks |
Early walking, large stature, obesity
|
Obesity |
| Classification |
Langenskiold |
No radiographic classification |
| Severity |
More severe physeal/epiphyseal disturbance |
Less severe physeal/epiphyseal disturbance |
| Location |
Physeal/epiphyseal |
Metaphyseal |
| Bone Involvement |
Proximal medial tibia physis, producing genu varus, flexion, internal rotation, AND may have compensatory distal femoral VALGUS |
Proximal tibia physis, AND may have distal femoral VARUS and distal tibia valgus |
| Natural History |
Self-limited - stage II and IV can exhibit spontaneous resolution |
Progressive, never resolves spontaneously (thus bracing unlikely to work) |
| Treatment Options |
Bracing and surgery
|
Surgery only |
|
| |
| Presentation |
- Physical exam
- hallmark is genu varum deformity
- obesity
- usually unilateral (compared to bilateral in infantile Blount's)
- limb-length discrepancy secondary to deformity
- mild to moderate laxity of medial collateral ligament
|
| Imaging |
- Radiographs

- views
- standing long-cassette AP radiograph of both lower extremities
- ensure patellas are facing forward (commonly associated with internal tibial torsion)
- findings suggestive of adolescent Blount's disease
- narrowing of the tibial epiphysis
- widening of the medial tibial growth plate
- occasional widening of the lateral distal femoral physis
- metaphyseal beaking less commonly seen with adolescent Blount's
- measurements
- metaphyseal-diaphyseal angle (Drennan)

- angle between line connecting metaphyseal beaks and a line perpendicular to the longitudinal axis of the tibia
- >16 degrees is considered abnormal
- tibiofemoral angle
- angle between the longitudinal axis of the femur and tibia
|
| Treatment |
- Nonoperative
- observation or bracing is unlikely to be successful - treatment is always surgical
- indications
- outcomes
- poor outcomes - will progresse and cause medial joint pain and altered kinematics
- early onset arthritis is common in untreated cases
- Operative
- lateral tibia and fibular epiphysiodesis
- indications
- mild to moderate deformity with growth remaining
- outcomes
- up to 25% may require formal osteotomy due to residual deformity
- proximal tibia/fibula osteotomy

- indications
- more severe cases in the skeletally mature
- outcomes
- multiplanar external fixation following osteotomy allows gradual angle and length correction and decreases risk on neurovascular structures
- distal femoral osteotomy or epiphysiodesis
- indications
- for distal femoral varus deformity of 8 degrees or greater
|
| Surgical Techniques |
- Lateral tibia and fibular epiphysiodesis
- transient hemiepiphysiodesis
- technique
- tether physis with 8-plates or staple
- may remove implant once correction is achieved
- pros
- simple
- allows for gradual correction is children with adequate growth remaining
- implants may be removed
- cons
- requires significant growth remaining
- close observation is necessary following operation as growth plate may stop functioning or have a rebound period of accelerated growth
- permanent hemiepiphysiodesis
- technique
- obliteration of physis through small, lateral incision
- pros
- limited surgery
- overcorrection is uncommon
- does not limit ability to perform corrective osteotomy in future
- cons
- cannot correct rotational deformity
- up to 25% may require formal corrective osteotomy
- Proximal tibia/fibula osteotomy
- goals of correction
- overcorrection to valgus not indicated (as is the case in infantile Blount's)
- strive for neutral mechanical axis
- high tibial osteotomy with rigid internal fixation
- technique
- variety of techniques, including closing wedge, opening wedge, dome, serrated and inclined osteotomies
- variety of fixation devices including cast, pins and wires, screws, plates and screws
- post-op
- limited weight bearing with use of crutches for 6-8 weeks
- pros
- cons
- potential for neurologic injury due to acute lengthening
- potential for compartment syndrome
- consider prophylactic fasciotomies
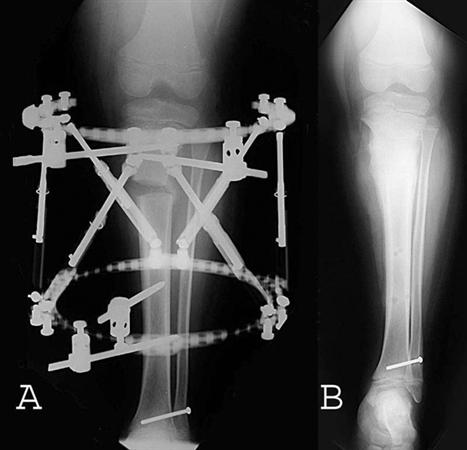
- osteotomy with external fixation and gradual correction
- technique
- perform osteotomy, and connect frame that allows for gradual correction
- Taylor Spatial Frame or Ilizarov ring external fixator

- post-op
- usually 12-18 weeks of treatment are needed
- pros
- gradual correction limits neurovascular compromise and risk for compartment syndrome
- allows for correction of deformity in all planes
- cons
- pin site infection
- duration of treatment
- bulk of construct
|