| Introduction |
- Mechanism typically high energy blunt trauma
- Mortality rate 15-25% for closed fractures, as much as 50% for open fractures
- hemorrhage is leading cause of death overall

- closed head injury is the most common for lateral compression injuries

- increased mortality associated with
- systolic BP <90 on presentation
- age >60 years
- increased Injury Severity Score (ISS) or Revised Trauma Score (RTS)
- need for transfusion > 4 units
- higher Young-Burgress classification grade

- Associated injuries
- chest injury in up to 63%
- long bone fractures in 50%
- sexual dysfunction up to 50%
- head and abdominal injury in 40%
- spine fractures in 25%
- Prognosis
- high prevalence of poor functional outcome and chronic pain
- poor outcome associated with
- SI joint incongruity of > 1 cm
- high degree initial displacement
- malunion or residual displacement
- leg length discrepancy > 2 cm
- nonunion
- neurologic injury
- urethral injury
- Pediatric pelvic ring fractures
- children with open triradiate cartilage have different fracture patterns than do children whose triradiate cartilage has closed
- if triradiate cartilage is open the iliac wing is weaker than the elastic pelvic ligaments, resulting in bone failure before pelvic ring disruption
- for this reason fractures usually involve the pubic rami and iliac wings and rarely require surgical treatment
|
| Anatomy |
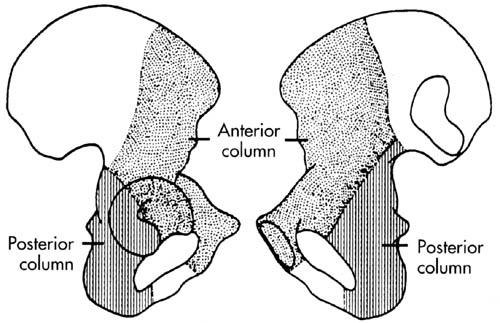
- Osteology
- ring structure made up of the sacrum and two innominate bones
- stability dependent on strong surrounding ligamentous structures
- displacement can only occur with disruption of the ring in two places
- neurovascular structures intimately associated with posterior pelvic ligaments

- high index of suspicion for injury of internal iliac vessels or lumbosacral plexus
- Ligaments
- anterior
- pelvic floor
- sacrospinous ligaments
- sacrotuberous ligaments
- posterior sacroiliac complex (posterior tension band)
- strongest ligaments in the body
- more important than anterior structures for pelvic ring stability
- anterior sacroiliac ligaments
- resist external rotation after failure of pelvic floor and anterior structures
- interosseous sacroiliac
- resist anterior-posterior translation of pelvis
- posterior sacroiliac
- resist cephalad-caudad displacement of pelvis
- iliolumbar
- resist rotation and augment posterior SI ligaments
|
| Physical Exam |
- Symptoms
- pain & inability to bear weight
- Physical exam
- inspection
- test stability by placing gentle rotational force on each iliac crest
- low sensitivity for detecting instability
- perform only once
- look for abnormal lower extremity positioning
- external rotation of one or both extremities

- limb-length discrepancy
- skin
- scrotal, labial or perineal hematoma, swelling or ecchymosis
- flank hematoma
- lacerations of perineum
- degloving injuries (Morel-Lavallee lesion)
- neurologic exam
- rule out lumbosacral plexus injuries (L5 and S1 are most common)
- rectal exam to evaluate sphincter tone and perirectal sensation
- urogenital exam
- most common finding is gross hematuria
- more common in males (21% in males, 8% in females)
- vaginal and rectal examinations
- mandatory to rule out occult open fracture
|
| Imaging |
- Radiographs
- recommended views
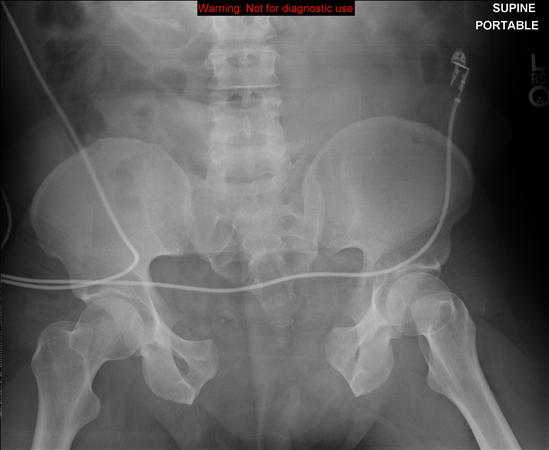
- AP
- part of initial ATLS evaluation
- look for asymmetry, rotation or displacement of each hemipelvis
- evidence of anterior ring injury needs further imaging
- inlet
- xray beam angled 40° caudad (may be as little as 25 degrees)
- adequate image when S1 overlaps S2 body
- ideal for visualizing
- anterior or posterior translation of the hemipelvis
- internal or external rotation of the hemipelvis
- widening of the SI joint
- sacral ala impaction
- outlet
- xray beam angled ~40° cephalad (may be as much as 60 degrees)
- adequate image when pubic symphysis overlies S2 body
- ideal for visualizing
- vertical translation of the hemipelvis
- flexion/extension of the hemipelvis
- disruption of sacral foramina and location of sacral fractures
- findings
- radiographic signs of instability
- > 5 mm displacement of posterior sacroiliac complex
- presence of posterior sacral fracture gap
- avulsion fractures (ischial spine, ischial tuberosity, sacrum, transverse process of 5th lumbar vertebrae)
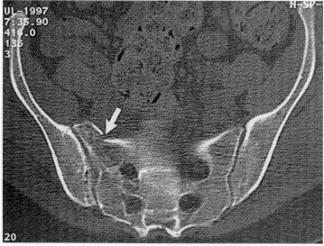
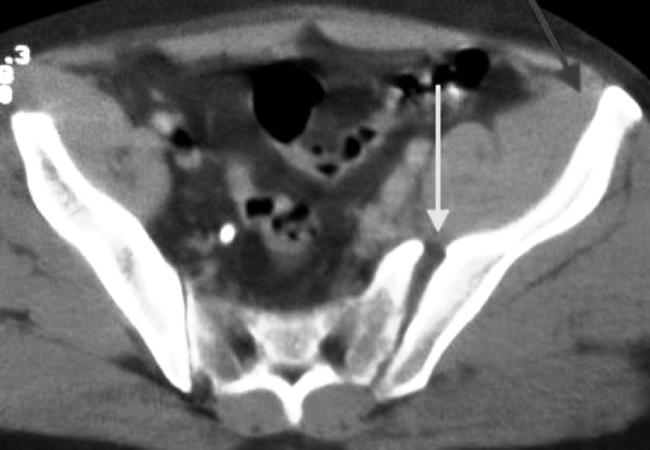
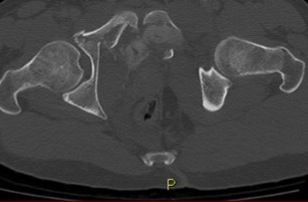
- CT
- routine part of pelvic ring injury evaluation
- better characterization of posterior ring injuries
- helps define comminution and fragment rotation
- visualize position of fracture lines relative to sacral foramina
|
| Classification & Treatment |
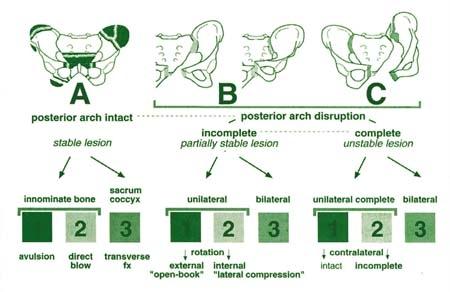
- Tile classification
- A: stable
- A1: fracture not involving the ring (avulsion or iliac wing fracture)
- A2: stable or minimally displaced fracture of the ring
- A3: transverse sacral fracture (Denis zone III sacral fracture)
- B - rotationally unstable, vertically stable
- B1: open book injury (external rotation)
- B2: lateral compression injury (internal rotation)
- B2-1: with anterior ring rotation/displacement through ipsilateral rami
- B2-2-with anterior ring rotation/displacement through contralateral rami (bucket-handle injury)
- B3: bilateral
- C - rotationally and vertically unstable
- C1: unilateral
- C1-1: iliac fracture
- C1-2: sacroiliac fracture-dislocation
- C1-3: sacral fracture
- C2: bilateral with one side type B and one side type C
- C3: bilateral with both sides type C
- Young-Burgess Classification
|
|
| Bleeding & Initial Treatment |
- Bleeding Source
- intraabdominal
- intrathoracic
- retroperitoneal
- extremity (thigh compartments)
- pelvic
- common sources of hemorrhage
- venous injury (80%)
- shearing injury of posterior thin walled venous plexus
- bleeding cancellous bone
- uncommon sources of hemorrhage
- arterial injury (10-20%)
- superior gluteal most common (posterior ring injury, APC pattern)
- internal pudendal (anterior ring injury, LC pattern)
- obturator (LC pattern)
- Treatment
- resuscitation
- PRBC:FFP:Platelets ideally should be transfused 1:1:1
- this ratio shown to improve mortality in patients requiring massive transfusion
- pelvic binder/sheet
- indications
- initial management of an unstable ring injury
- contraindications
- hypothetical risk of over-rotation of hemipelvis and hollow viscus injury (bladder) in pelvic fractures with internal rotation component (LC)
- no clinical evidence exists of this complication occurring
- technique
- centered over greater trochanters to effect indirect reduction
- do not place over iliac crest/abdomen
- ineffective and precludes assessment of abdomen
- may augment with internal rotation of lower extremities and taping at ankles
- transition to alternative fixation as soon as possible
- prolonged pressure from binder or sheet may cause skin necrosis
- working portals may be cut in sheet to place percutaneous fixation
- pitfalls
- binder can mask pelvic ring injuries, creating false negative radiographs and CT images
- stress examination under anesthesia may be indicated in patients who present to the trauma slot in a pelvic binder, hemodynamic instability, and negative pelvis radiographs/CT scan
- external fixation
- indications
- pelvic ring injuries with an external rotation component (APC, VS, CM)
- unstable ring injury with ongoing blood loss
- contraindications
- ilium fracture that precludes safe application
- acetabular fracture
- technique
- theoretically works by decreasing pelvic volume
- stability of bleeding bone surfaces and venous plexus in order to form clot
- pins inserted into ilium
- supra-acetabular pin insertion
- single pin in column of supracetabular bone from AIIS towards PSIS
- obturator outlet view
- helps to identify pin entry point
- iliac oblique view
- helps to direct pin above greater sciatic notch
- obturator oblique inlet view
- helps to ensure pin placement within inner and outer table
- AIIS pins can place the lateral femoral cutaneous nerve at risk
- pedicle screws with internal subcutaneous bar may be used
- superior iliac crest pin insertion
- multiple half pins in the superior iliac crest
- place in thickest portion of ilium (gluteal pillar)
- may be placed with minimal fluoroscopy
- should be placed before emergent laparotomy
- angiography / embolization
- indications
- controversial and based on multiple variables including:
- protocol of institution, stability of patient, proximity of angiography suite , availability and experience of IR staff
- CT angiography useful for determining presence or absence of ongoing arterial hemorrhage (98-100% negative predictive value)
- contraindications
- technique
- selective embolization of identifiable bleeding sources
- in patients with uncontrolled bleeding after selective embolization, bilateral temporary internal iliac embolization may be effective
- complications include gluteal necrosis and impotence
|
| Definitive Treatment |
- Nonoperative
- weight bearing as tolerated
- indications
- mechanically stable pelvic ring injuries including
- LC1
- anterior impaction fracture of sacrum and oblique ramus fractures with < 1cm of posterior ring displacement
- APC1
- widening of symphysis < 2.5 cm with intact posterior pelvic ring
- isolated pubic ramus fractures
- parturition-induced pelvic diastasis
- bedrest and pelvic binder in acute setting with diastasis less than 4cm
- Operative
- ORIF
- indications
- symphysis diastasis > 2.5 cm
- SI joint displacement > 1 cm
- sacral fracture with displacement > 1 cm
- displacement or rotation of hemipelvis
- open fracture
- chronic pain and diastasis in parturition-induced diastasis or acute setting >6cm
- technique
- for open fractures aggressive debridement according to open fracture principles
- anterior subcutaneous pelvic fixator (INFIX)
- indications
- same indications as anterior external fixation and symphyseal plating
- complications
- heterotopic ossification, femoral nerve injury, infection
- diverting colostomy
- indications
- consider in open pelvic fractures
- especially with extensive perineal injury or rectal involvement
|
| Techniques |
- Anterior ring stabilization
- single superior plate
- apply through rectus-splitting Pfannenstiel approach
- may perform in conjunction with laparotomy or GU procedure
- Posterior ring stabilization
- anterior SI plating
- risk of L4 and L5 injury with placement of anterior sacral retractors
- iliosacral screws (percutaneous)
- good for sacral fractures and SI dislocations
- safe zone is in S1 vertebral body
- outlet radiograph view best guides superior-inferior screw placement
- inlet radiograph view best guides anterior-posterior screw placement
- L5 nerve root injury complication with errors in screw placement
- entry point best viewed on lateral sacral view and pelvic outlet views
- risk of loss of reduction highest in vertical sacral fracture patterns
- posterior SI "tension" plating
- can have prominent HW complications
- Anterior and posterior ring stabilization
- necessary in vertically unstable injuries
- Ipsilateral acetabular and pelvic ring fractures
- reduction and fixation of the pelvic ring should be performed first
|
| Complications |
- Neurologic injury
- L5 nerve root runs over sacral ala joint
- may be injured if SI screw is placed to anterior
- anterior subcutaneous pelvic fixator may give rise to LFCN injury (most common) or femoral nerve injury
- DVT and PE
- DVT in ~ 60%, PE in ~ 27%
- prophylaxis essential
- mechanical compression
- pharmacologic prevention (LMWH or Lovenox)
- vena caval filters (closed head injury)
- Chronic instability
- rare complication; can be seen in nonoperative cases
- presents with subjective instability and mechanical symptoms
- diagnosed with alternating single-leg-stance pelvic radiographs
- Infection
- risk factors include:
- obesity
- diabetes
- delay in treatment
- open fracture
|
| Urogenital Injuries |
- Present in 12-20% of patients with pelvic fractures
- higher incidence in males (21%)
- Includes
- posterior urethral tear
- most common urogenital injury with pelvic ring fracture
- bladder rupture
- may see extravasation around the pubic symphysis

- associated with mortality of 22-34%
- Diagnosis
- made with retrograde urethrocystogram
- indications for retrograde urethrocystogram include
- blood at meatus
- high riding or excessively mobile prostate
- hematuria
- Treatment
- suprapubic catheter placement
- suprapubic catheter is a relative contraindication to anterior ring plating
- surgical repair
- rupture should be repaired at the same time or prior to definitive fixation in order to minimize infection risk
- Complications
- long-term complications common (up to 35%)
- urethral stricture - most common
- impotence
- anterior pelvic ring infection
- incontinence
- parturition sequelae (i.e. caesarean section)
|