| Introduction | |
|
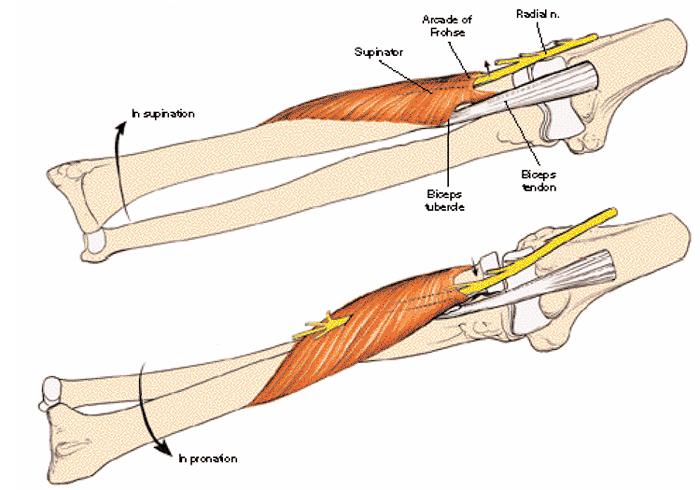
| Anatomy | |||||||||||||||
|
|||||||||||||||
| Classification | |||||||||||||||
|
|||||||||||||||
| Presentation | |||||||||||||||
|
|||||||||||||||
| Imaging | |||||||||||||||
|
|||||||||||||||
| Treatment | |||||||||||||||
|
|||||||||||||||
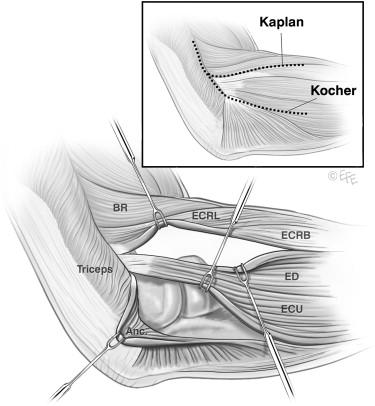
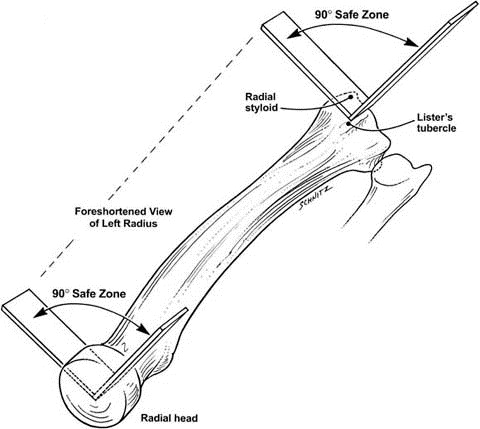
| Techniques | |||||||||||||||
|
|||||||||||||||
| Introduction | |
|
| Anatomy | |||||||||||||||
|
|||||||||||||||
| Classification | |||||||||||||||
|
|||||||||||||||
| Presentation | |||||||||||||||
|
|||||||||||||||
| Imaging | |||||||||||||||
|
|||||||||||||||
| Treatment | |||||||||||||||
|
|||||||||||||||
| Techniques | |||||||||||||||
|
|||||||||||||||
جميع البيانات و المستندات الموجوده لكل موقع من مواقع الاعضاء تقع صحتها قانونيا و أدبيا على العضو نفسه